Looking for PALS H’s and T’s go HERE.
Knowing the H’s and T’s of ACLS will help prepare you for any ACLS scenario. The H’s and T’s of ACLS is a mnemonic used to help recall the major contributing factors to pulseless arrest including PEA, Asystole, Ventricular Fibrillation, and Ventricular Tachycardia. These H’s and T’s will most commonly be associated with PEA, but they will help direct your search for underlying causes to any of arrhythmias associated with ACLS. Each is discussed more thoroughly below.
Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hyper-/hypokalemia, Hypoglycemia, Hypothermia.
Toxins, Tamponade(cardiac),Tension pneumothorax, Thrombosis (coronary and pulmonary), and Trauma.
The H’s include:
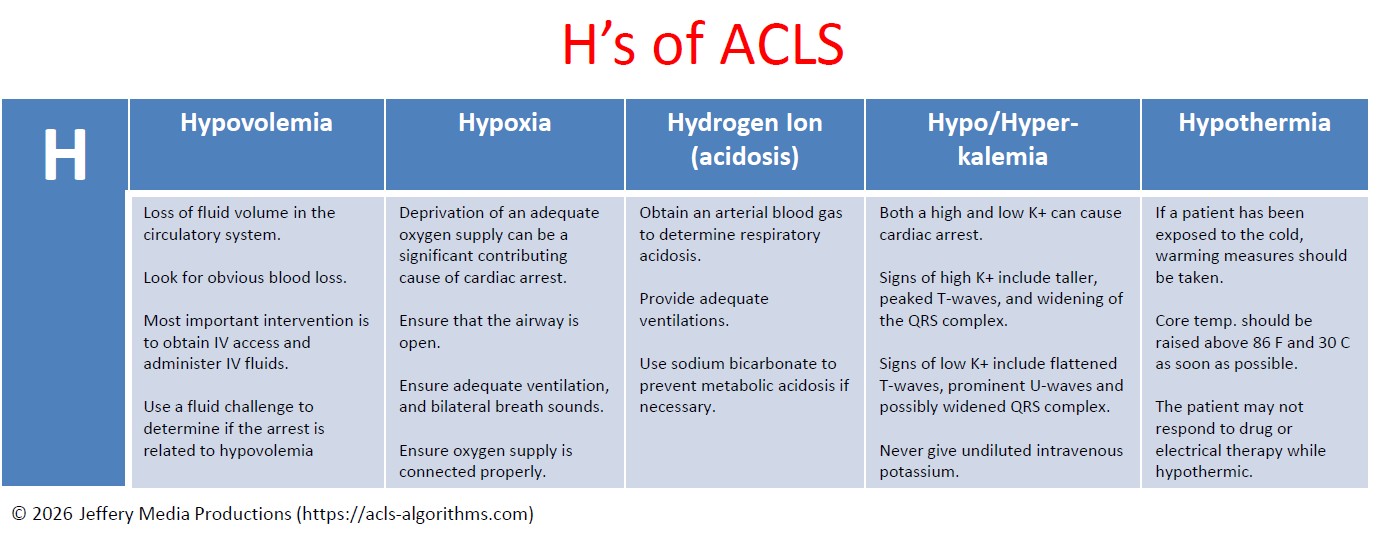
Hypovolemia
Hypovolemia or the loss of fluid volume in the circulatory system can be a major contributing cause of cardiac arrest. Looking for obvious blood loss in the patient with pulseless arrest is the first step in determining if the arrest is related to hypovolemia. After CPR, the most important intervention is obtaining intravenous access/IO access. A fluid challenge or fluid bolus may also help determine if the arrest is related to hypovolemia.
Hypoxia
Hypoxia or deprivation of adequate oxygen supply can be a significant contributing cause of cardiac arrest. You must ensure that the patient’s airway is open and that the patient has chest rise and fall and bilateral breath sounds with ventilation. Also, ensure that your oxygen source is connected properly.
Hydrogen ion (acidosis)
To determine if the patient is in respiratory acidosis, an arterial blood gas evaluation must be performed. Prevent respiratory acidosis by providing adequate ventilation. Prevent metabolic acidosis by giving the patient sodium bicarbonate.
Hyper-/hypokalemia
Both a high potassium level and a low potassium level can contribute to cardiac arrest. The major sign of hyperkalemia or high serum potassium is taller and peaked T-waves. Also, a widening of the QRS-wave may be seen. This can be treated in a number of ways which include sodium bicarbonate (IV), glucose+insulin, calcium chloride (IV), Kayexalate, dialysis, and possibly albuterol. All of these will help reduce serum potassium levels. Read more about hyperkalemia with cardiac arrest here.
The major signs of hypokalemia or low serum potassium are flattened T-waves, prominent U-waves, and possibly a widened QRS complex. Treatment of hypokalemia involves rapid but controlled infusion of potassium. Giving IV potassium has risks. Always follow the appropriate infusion standards. Never give undiluted intravenous potassium.
Hypoglycemia
Hypoglycemia or low serum blood glucose can have many negative effects on the body, and it can be associated with cardiac arrest. Treat hypoglycemia with IV dextrose to reverse a low blood glucose. Hypoglycemia was removed from the H’s but is still to be considered important during the assessment of any person in cardiac arrest.
Hypothermia
If a patient has been exposed to the cold, warming measures should be taken. The hypothermic patient may be unresponsive to drug therapy and electrical therapy (defibrillation or pacing). Core temperature should be raised above 86 F (30 C) as soon as possible.
The T’s include:
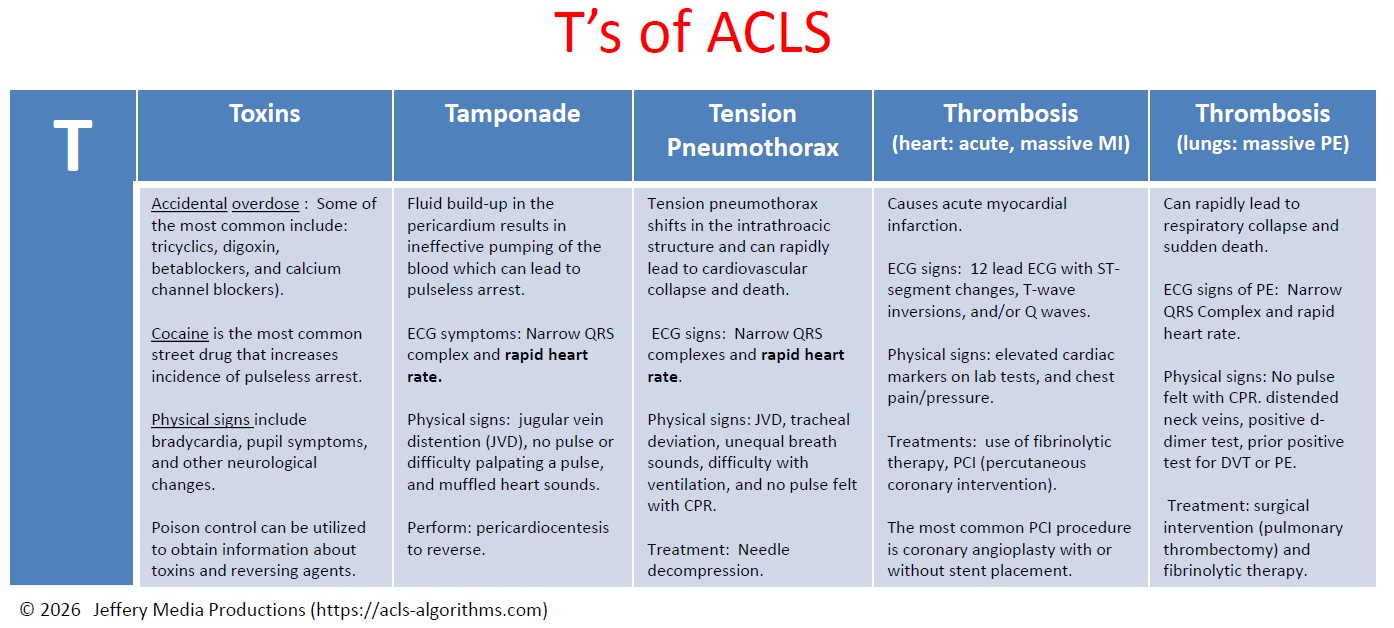
Toxins
Accidental overdose of a number of different kinds of medications can cause pulseless arrest. Some of the most common include tricyclics, digoxin, beta-blockers, and calcium channel blockers. Street drugs and other chemicals can precipitate pulseless arrest. Cocaine is the most common street drug that increases the incidence of pulseless arrest. ECG signs of toxicity include prolongation of the QT interval. Signs of toxicity include bradycardia, pupil symptoms, and other neurological changes. Support of circulation while an antidote or reversing agent is obtained is of primary importance. Poison control can be utilized to obtain information about toxins and reversing agents.
Tamponade
Cardiac tamponade is an emergency condition in which fluid accumulates in the pericardium (sac in which the heart is enclosed). The buildup of fluid results in the ineffective pumping of the blood which can lead to cardiac arrest. ECG symptoms include narrow QRS complex and rapid heart rate. Physical signs include jugular vein distention (JVD), no pulse or difficulty palpating a pulse, and muffled heart sounds due to the fluid inside the pericardium. The recommended treatment for cardiac tamponade is pericardiocentesis.
Tension Pneumothorax
Tension pneumothorax occurs when air is allowed to enter the pleural space and is prevented from escaping naturally. This leads to a build-up of tension that causes shifts in the intrathoracic structure that can rapidly lead to cardiovascular collapse and death. ECG signs include narrow QRS complexes and rapid heart rate. Physical signs include JVD, tracheal deviation, unequal breath sounds, difficulty with ventilation, and no pulse felt with CPR. Treatment of tension pneumothorax is needle decompression.
Thrombosis (heart: acute, massive MI)
Coronary thrombosis is an occlusion or blockage of blood flow within a coronary artery caused by blood that has clotted within the vessel. The clotted blood causes an acute myocardial infarction which destroys heart muscle and can lead to sudden death depending on the location of the blockage.
ECG signs during PEA indicating coronary thrombosis include ST-segment changes, T-wave inversions, and/or Q waves. Physical signs include elevated cardiac markers on lab tests.
For patients with cardiac arrest and without known pulmonary embolism (PE), routine fibrinolytic treatment given during CPR has shown no benefit and is not recommended.
Treatments for coronary thrombosis before cardiac arrest include the use of fibrinolytic therapy, or PCI (percutaneous coronary intervention). The most common PCI procedure is coronary angioplasty with or without stent placement.
Thrombosis (lungs: massive pulmonary embolism)
Pulmonary thrombus or pulmonary embolism (PE) is a blockage of the main artery of the lung which can rapidly lead to respiratory collapse and sudden death. ECG signs of PE include narrow QRS Complex and rapid heart rate. Physical signs include no pulse felt with CPR. distended neck veins, positive d-dimer test, prior positive test for DVT or PE. Treatment includes surgical intervention (pulmonary thrombectomy) and fibrinolytic therapy.
Trauma
The final differential diagnosis of the H’s and T’s is trauma. Trauma can be a cause of pulseless arrest, and a proper evaluation of the patient’s physical condition and history should reveal any traumatic injuries. Treat each traumatic injury as needed to correct any reversible cause or contributing factor to the pulseless arrest. Trauma was removed from the T’s but is still to be considered important during the assessment of any person in cardiac arrest.
Barbara Thomas says
I have acls tomorrow like this site for review . thanks
Jeff with admin. says
You are welcome. Best wishes with your ACLS tomorrow. Kind Regards, Jeff
Rochelle Radcliff says
Thanks for the H’s and T’s chart. One of the best I’ve seen.
Elaine McKinney says
Thank You for the H and T chart it is great.
Marcia Heng says
Hi Jeff,
Thank you for taking the time to put this website together as you have.
In my opinion, it is the best online website program for ACLS preparation.
You utilize the best learning methods for us healthcare workers to learn and retain the information – Clear, Concise, Consistent accurate information with an emphasize on repetition. Thanks!
On another note, I have a question for you,
At some point as I was going through the site I thought I came across two supplemental tables for the H’s & T’s. It’s not the two that are currently listed under H’s and T’s section (H one that starts with loss of fluid and T one that starts with accidental overdose). Do you know what I am referring to? Are there anymore tables for the ACLS H’s and T’s besides those two? Thank you!
Jeff with admin. says
Hi Marcia,
Thanks for your encouragement. I’m so glad that the site has been helpful for you.
I think you may be referring to the downloadable PDF for the H’s and T’s can find that here: Downloadable PDF
Kind Regards, Jeff
Arya Bima says
WHY hypoglycemia and trauma was removed from Hs and Ts?
If both of them are still to be considered important during the assessment of any person in cardiac arrest, then they must be included in Hs and Ts. Am I right?
Jeff with admin. says
American Heart Association removed hypoglycemia and trauma from the Hs and Ts in order to continue to further simplify advanced cardiac life support.
Honestly, I think it was a poor decision to remove them, and I would not be surprised if they are added back in the future.
It seems to me that there are many better ways to simplify ACLS then removing them from the Hs and Ts.
Kind regards,
Jeff
Alec says
Why not remove Thrombosis, as there is no way to asses or diagnose/treat pulmonary or cardiac thrombosis in an unresponsive pt.
Jeff with admin. says
The main reason would be so that you could properly rule out other causes. Even though thrombosis may not be easy to treat, it’s identification would assist in providing appropriate interventions.
The earlier that thrombosis is identified, the higher the potential for a positive outcome. Sometimes this can even be recognized in the prearrest phase when providers are keenly aware of symptoms that occur.
Kind regards,
Jeff
Peter says
There is no evidence that hypoglycemia causes direct cardiac arrest. There is some evidence that shows hypoglycemia can cause long QT which in turn can result in VF. We know hypoglycemia can result in respiratory depression/ loss of airway- this may result in hypoxia which is a known cause of arrest. Evidence found dextrose admin in cardiac arrest resulted in increased rate of ROSC but decrease survival to hosp dicharges and those who do survive have poorer outcomes.
Poor perfusion states such as cardiac arrest results in very inacurate finger prick readings. Less than 30% who tested hypo was actually hypo.
https://www.ncbi.nlm.nih.gov/pubmed/17763842
https://www.ncbi.nlm.nih.gov/pubmed/2029097
Don’t have link at hand for rest of evidence, quick google search should pop them up.
Our approach is once you have ROSC, check sugar, correct if needed. Post VF arrest commonly results in hyperglycemia for initial period post arrest (in absence of glucose administration)
Jeff with admin. says
Thank you for sharing this. Kind regards, Jeff
nanette gormley says
what is pea
Jeff with admin. says
PEA means pulseless electrical activity. PEA is addressed in the right branch of the cardiac arrest algorithm how long with asystole.
Kind regards, Jeff
Mukesh Nangia says
Great site. I will recommend it to my colleagues.
Jeni says
I am a pediatric cardiac nurse. I’m reviewing your website while I am home in bed with the flu. I think your information is presented in a way that is easy to comprehend. I will be recommending your site to my fellow nurses, pct’s, and telemetry techs on my unit. Thanks!
Elizabeth Tichy says
As a nursing student in my final semester, this site is AMAZING!! Thank you, Sir!!
Respectfully,
Elizabeth T.
Alniren says
I have only till tom to review, I did my acls pretest andI got 96%. I feel more comfortable now, this reviewer is very helpful and very informative. I recommended this website to my coworkers. I will definitely use this again in the future!
Jeff with admin. says
Thank you for the encouragement. I’m so glad that the site has been helpful for you. Kind regards, Jeff
cancelm5 says
hello… I am taking ACLS (part 2 and test) next week and I am hoping this will help me out!! This site is of great help in reviewing this material. Thank you… I also shared this site with my colleagues that are taking the testing with me! MC
Jeff with admin. says
You are very welcome. You will do great with the certification. Let me know how things go.
Also, thanks for sharing the site with you colleagues.
Kind regards,
Jeff
Rchaplea says
Excellent review, especially appreciated the h’s and t’s charts.
Lizymaurice says
Much useful information.
Thanks a lot for uploading.
koome says
Thankyou for update. AHA recommendation on acls still remains the best.
crolik207 says
Hi Jeff,
Quick question. When will we see an undiluted potassium medication? Usually the potassium that the hospital carries is potassium chloride with for example 20 meqs and I am sure that is considered diluted. Is this correct?
Thank in advance.
Jeff with admin. says
You will not ever see undiluted potassium. Undiluted potassium when injected intravenously is lethal.
If potassium level is < 3 and the patient is symptomatic, 40 meq/hour may be administered to intensive care patients. That is the maximum infusion rate per hour. Kind regards, Jeff