Looking for PALS H’s and T’s go HERE.
Knowing the H’s and T’s of ACLS will help prepare you for any ACLS scenario. The H’s and T’s of ACLS is a mnemonic used to help recall the major contributing factors to pulseless arrest including PEA, Asystole, Ventricular Fibrillation, and Ventricular Tachycardia. These H’s and T’s will most commonly be associated with PEA, but they will help direct your search for underlying causes to any of arrhythmias associated with ACLS. Each is discussed more thoroughly below.
Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hyper-/hypokalemia, Hypoglycemia, Hypothermia.
Toxins, Tamponade(cardiac),Tension pneumothorax, Thrombosis (coronary and pulmonary), and Trauma.
The H’s include:
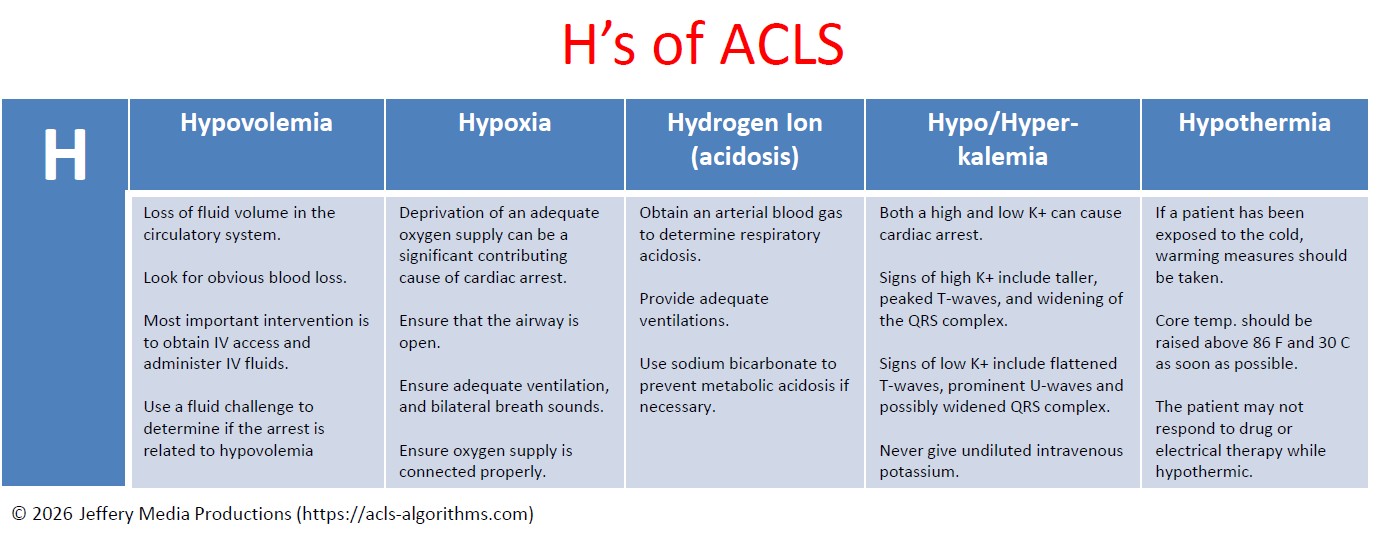
Hypovolemia
Hypovolemia or the loss of fluid volume in the circulatory system can be a major contributing cause of cardiac arrest. Looking for obvious blood loss in the patient with pulseless arrest is the first step in determining if the arrest is related to hypovolemia. After CPR, the most important intervention is obtaining intravenous access/IO access. A fluid challenge or fluid bolus may also help determine if the arrest is related to hypovolemia.
Hypoxia
Hypoxia or deprivation of adequate oxygen supply can be a significant contributing cause of cardiac arrest. You must ensure that the patient’s airway is open and that the patient has chest rise and fall and bilateral breath sounds with ventilation. Also, ensure that your oxygen source is connected properly.
Hydrogen ion (acidosis)
To determine if the patient is in respiratory acidosis, an arterial blood gas evaluation must be performed. Prevent respiratory acidosis by providing adequate ventilation. Prevent metabolic acidosis by giving the patient sodium bicarbonate.
Hyper-/hypokalemia
Both a high potassium level and a low potassium level can contribute to cardiac arrest. The major sign of hyperkalemia or high serum potassium is taller and peaked T-waves. Also, a widening of the QRS-wave may be seen. This can be treated in a number of ways which include sodium bicarbonate (IV), glucose+insulin, calcium chloride (IV), Kayexalate, dialysis, and possibly albuterol. All of these will help reduce serum potassium levels. Read more about hyperkalemia with cardiac arrest here.
The major signs of hypokalemia or low serum potassium are flattened T-waves, prominent U-waves, and possibly a widened QRS complex. Treatment of hypokalemia involves rapid but controlled infusion of potassium. Giving IV potassium has risks. Always follow the appropriate infusion standards. Never give undiluted intravenous potassium.
Hypoglycemia
Hypoglycemia or low serum blood glucose can have many negative effects on the body, and it can be associated with cardiac arrest. Treat hypoglycemia with IV dextrose to reverse a low blood glucose. Hypoglycemia was removed from the H’s but is still to be considered important during the assessment of any person in cardiac arrest.
Hypothermia
If a patient has been exposed to the cold, warming measures should be taken. The hypothermic patient may be unresponsive to drug therapy and electrical therapy (defibrillation or pacing). Core temperature should be raised above 86 F (30 C) as soon as possible.
The T’s include:
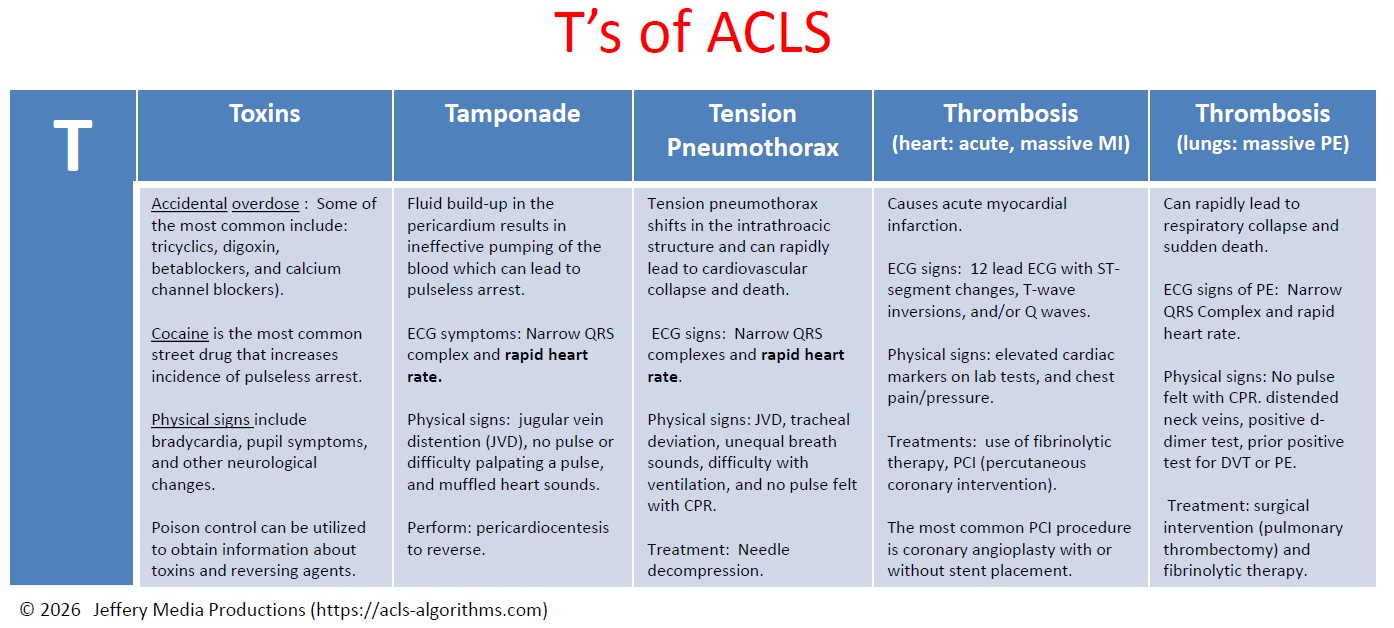
Toxins
Accidental overdose of a number of different kinds of medications can cause pulseless arrest. Some of the most common include tricyclics, digoxin, beta-blockers, and calcium channel blockers. Street drugs and other chemicals can precipitate pulseless arrest. Cocaine is the most common street drug that increases the incidence of pulseless arrest. ECG signs of toxicity include prolongation of the QT interval. Signs of toxicity include bradycardia, pupil symptoms, and other neurological changes. Support of circulation while an antidote or reversing agent is obtained is of primary importance. Poison control can be utilized to obtain information about toxins and reversing agents.
Tamponade
Cardiac tamponade is an emergency condition in which fluid accumulates in the pericardium (sac in which the heart is enclosed). The buildup of fluid results in the ineffective pumping of the blood which can lead to cardiac arrest. ECG symptoms include narrow QRS complex and rapid heart rate. Physical signs include jugular vein distention (JVD), no pulse or difficulty palpating a pulse, and muffled heart sounds due to the fluid inside the pericardium. The recommended treatment for cardiac tamponade is pericardiocentesis.
Tension Pneumothorax
Tension pneumothorax occurs when air is allowed to enter the pleural space and is prevented from escaping naturally. This leads to a build-up of tension that causes shifts in the intrathoracic structure that can rapidly lead to cardiovascular collapse and death. ECG signs include narrow QRS complexes and rapid heart rate. Physical signs include JVD, tracheal deviation, unequal breath sounds, difficulty with ventilation, and no pulse felt with CPR. Treatment of tension pneumothorax is needle decompression.
Thrombosis (heart: acute, massive MI)
Coronary thrombosis is an occlusion or blockage of blood flow within a coronary artery caused by blood that has clotted within the vessel. The clotted blood causes an acute myocardial infarction which destroys heart muscle and can lead to sudden death depending on the location of the blockage.
ECG signs during PEA indicating coronary thrombosis include ST-segment changes, T-wave inversions, and/or Q waves. Physical signs include elevated cardiac markers on lab tests.
For patients with cardiac arrest and without known pulmonary embolism (PE), routine fibrinolytic treatment given during CPR has shown no benefit and is not recommended.
Treatments for coronary thrombosis before cardiac arrest include the use of fibrinolytic therapy, or PCI (percutaneous coronary intervention). The most common PCI procedure is coronary angioplasty with or without stent placement.
Thrombosis (lungs: massive pulmonary embolism)
Pulmonary thrombus or pulmonary embolism (PE) is a blockage of the main artery of the lung which can rapidly lead to respiratory collapse and sudden death. ECG signs of PE include narrow QRS Complex and rapid heart rate. Physical signs include no pulse felt with CPR. distended neck veins, positive d-dimer test, prior positive test for DVT or PE. Treatment includes surgical intervention (pulmonary thrombectomy) and fibrinolytic therapy.
Trauma
The final differential diagnosis of the H’s and T’s is trauma. Trauma can be a cause of pulseless arrest, and a proper evaluation of the patient’s physical condition and history should reveal any traumatic injuries. Treat each traumatic injury as needed to correct any reversible cause or contributing factor to the pulseless arrest. Trauma was removed from the T’s but is still to be considered important during the assessment of any person in cardiac arrest.
Dominick Walenczak says
Based on the evidence from Peng, et al, 2015… we should probably not be treating hypoglycemia during cardiac arrest as Dextrose administration was associated with worse survival and neurologic outcomes and no significant impact on obtaining ROSC. Glucose isn’t the primary source of myocardial ATP anyways.
Paulo Kraemer says
Hi Dominick,
What would be the primary source of myocardial ATP if it is not glucose?
Thanks,
Paulo Kraemer
paigeowenRN says
It’s fatty acids that provide the most ATP. However, considering that we can’t really give someone a rapid fish oil infusion, glucose is a less optimal, but readily available intervention in an effort to try to generate ATP.
The Peng, et all study did bring about the concern for the effect of dextrose used during in-hospital cardiac arrest patients, but could not establish a causal relationship between administration and lower survival rates… Definitely an interesting question. If anything, it encourages to establish the rationale verses doing things “they way we’ve always done it.”
With so many multi-variable factors contributing to cardiac arrests, it’s no doubt a challenging task to prove EBP in arrest management…
Manuel Lam says
Instead of dextrose administration, it would be interesting to investigate the administration of ketone esters for in-hospital cardiac arrest patients.
Jeckson Mureri says
Hi Jeffy
Is there any difference between ACLS offered by AHA and the one from APC ( American Physicians College)?
Can you sit for either of exams after studying through this website?
And which one is better between these two?
Jeff with admin. says
There’s a big difference. Most hospitals only except American Heart Association ACLS provider card. The American physicians college ACLS is avery questionable ACLS certification. This is true for any online ACLS course.
I recommend that you check with your education department and find out what ACLS course is they will accept. Most will only accept AHA.
As a sidenote, I checked the ranking status of the American College of physicians on the web. The rank status basically tells how important the website is compared to other websites. It was ranked very poorly. Out of all the websites on the Internet, it was ranked over 14 millionth. The closer the number to the #1, the better the ranking. Any website ranked less than about 1 million is invisible on the web unless they advertise.
Be careful with this website and make sure that anything that comes from it will be accepted by your employer.
Kind regards,
Jeff
David 576 says
Hi I’m guessing this is the American version of H’s and T’s as we still,have trauma and hypoglycaemia as part of out H&T’s
Jeff with admin. says
According to AHA guidelines, trauma is no longer included in the H and T’s and is included in the “Special circumstances of resuscitation.”
Hypoglycemia was removed because there is not sufficient evidence to support its being a cause of PEA or Asystole. It is also considered standard of practice to always check a blood sugar to ensure hypoglycemia is not present.
Kind regards,
Jeff
Emmily Tkach says
Dear Jeff,
Can you please explain why bradycardia would be present in a tension pneumothorax?
Thanks
Jeff with admin. says
The bradycardia could simply be an impending late sign of cardiovascular collapse related to tension pneumothorax. Also, tension pneumothorax can stimulate the vagus nerve and cause hypervagotonia leading to sinus bradycardia. Kind regards, Jeff
john says
Thanks so much for infor. Mostly by explaining why trauma and hypoglyxaemia removed.
Stevenlesser says
100% navy quality review,thanks
S H L md
Franklin says
A good refresher for the morning. Thanks!!
Devin says
Can you provide some insight as to why hypoglycemia and trauma removed from the Hs and Ts?
Cheers!
Jeff with admin. says
AHA has removed these from the H and T’s for the following reasons:
Trauma now has it own specific treatment recommendations within AHA ACLS protocol under special resuscitation situations.
Hypoglycemia was removed because the blood glucose check is now a routine standard that is expected to be done with any changes in level of consciousness. It is still very important and should not be neglected.
Kind regards,
Jeff
Paulo Kraemer says
Hi Jeff,
I understand that hypoglycemia was removed from the list as a cause of cardiac arrest because the blood glucose check is now a routine standard that is expected to be done with any changes in level of consciousness. The patient under cardiac arrest is, obviously, unconscious (not responding).
My questions are:
1) Should blood glucose level be checked during the CPR?
2) If so, what would be the most appropriate moment to check blood glucose during CPR?
3) Once checked during CPR, and the patient is said hypoglycemic, would it be wise (or indicated) to give IV glucose in order to correct the hypoglycemic state during CPR?
Thank you.
Jeff with admin. says
1. Yes, a blood sugar should be checked during CPR.
2. As soon as possible.
3. Yes, the hypoglycemic state should be initally treated with 1 amp IV D50 push.
Kind regards,
Jeff
Paulo Kraemer says
Hi, Jeff
I agree with yours answers about he importance of checking and managing hypoglycemia during CPR , but my concern is that this is not stated in the AHA CPR Guidelines.
Jacky says
Very useful information.
Thank you a lot
Lutfismiles says
Thank you!
anandu says
why u remove hypoglycemia from the algorithm
Jeff with admin. says
Hypoglycemia was removed because the blood glucose check is now a routine standard that is expected to be done with any changes in level of consciousness. It is still very important and should not be neglected.
Kind regards,
Jeff
jai says
thanks alot for invalueble info
Hashim Al-Mashagbih says
Thanks a lot for these information…
Jessica Rose says
I apologize if this has been covered somewhere else before, but is there any particular reasoning behind removing Hypoglycemia and Trauma from the list of H’s and T’s? I haven’t been able to find any reasoning or research that supports the removal of these items and It seems to me that these factors are still very valid in Cardiac assessments.
Thanks for the help!
Jeff with admin. says
AHA has removed these from the H and T’s for the following reasons:
Trauma now has it own specific treatment recommendations within AHA ACLS protocol under special resuscitation situations.
Hypoglycemia was removed because the blood glucose check is now a routine standard that is expected to be done with any changes in level of consciousness. It is still very important and should not be neglected.
Kind regards,
Jeff
Jessica Rose says
Makes sense! Thank you for explaining!
Wendy says
Amazing , helpful , and very good info. Very helpful study guide and simulations! Highly recommended.
Thank you.
Antonio says
Amazing resume information.
Thanks a lot.
So helpful.