High serum potassium levels (hyperkalemia) can be life-threatening and requires immediate therapy. There are several conditions which can significantly affect serum potassium levels and cause them to rise.
The amount of potassium (K+) in the blood determines the excitability of nerve and muscle cells, including the heart muscle or myocardium. When potassium levels in the blood rise, this reduces the electrical potential and can lead to potentially fatal abnormal heart rhythms.
Causes of High Serum Potassium
Metabolic acidosis causes a decrease in serum pH which has a direct effect on serum potassium levels. When serum pH drops (metabolic acidosis) serum potassium rises, and potassium shifts from intracellular to extracellular (into the blood).
Another condition that is a common cause of hyperkalemia is end-stage renal disease. When the kidneys fail, excess potassium cannot be removed, and it accumulates in the blood.
Signs and symptoms of hyperkalemia include weakness, ascending paralysis, and respiratory failure.
Signs and Symptoms
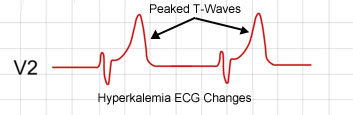
There are some ECG signs that may suggest hyperkalemia. Mild hyperkalemia can cause peaked T waves.
As potassium levels continue to rise, there may be flattened p-waves, a prolonged PR-interval, and other anomalies. If hyperkalemia is left untreated idioventricular rhythms may occur and a sine-wave pattern. 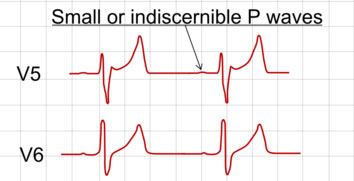 Severe hyperkalemia can lead to asystolic cardiac arrest.
Severe hyperkalemia can lead to asystolic cardiac arrest.
Treatment and Management
The treatment of hyperkalemia depends on the severity and the patient’s clinical presentation.
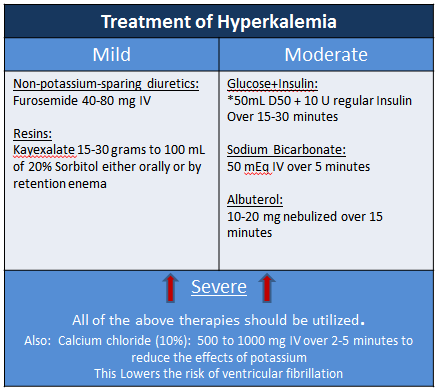
For mild hyperkalemia removal of potassium from the body is achieved with diuretics which cause the release of potassium in the urine. One example of a diuretic which does not spare potassium is furosemide.
Resins like Kayexalate can also be used to remove potassium from the body. Kayexalate can be administered orally or by retention enema.
For moderate elevation, potassium can be shifted from the vascular space (serum) to intracellular space using the 3 methods listed below:
- The administration of glucose + insulin (50ml D50 + 10 units regular insulin) can be given over 5 minutes. The onset of effect will take 15-30 min.
- Nebulized albuterol: 10 to 15 mg nebulized over 15 minutes
- Sodium Bicarbonate: 50 mEq IV over 5 minutes.
For severe elevation, both removal of potassium from the body and shifting potassium to the intracellular space is critical. The measures listed above in each category should be utilized. Along with this, Calcium Chloride should be given over 2 to 5 minutes to reduce the effects of high potassium levels on the heart. When hyperkalemia is severe, administration of calcium chloride lowers the risk of ventricular fibrillation.
The table below contains the medications listed above and their most common dosages.
Rayna says
Hi, does calcium chloride have to be diluted when you are pushing it in a code?
ACLS says
Calcium chloride does not necessarily have to be diluted when administered during a cardiac arrest (code) situation, but there are important considerations to keep in mind:
During a cardiac arrest, calcium chloride 10% solution can be administered undiluted as a slow intravenous push. The typical adult dose ranges from 500 mg to 1 g (5 to 10 mL of 10% solution).
Even when given undiluted, calcium chloride should be administered slowly:
• The injection rate should not exceed 1 mL/min.
• Some sources recommend administering over 2-5 minutes.
When administering undiluted calcium chloride:
Use a large vein, preferably central or deep.
• Avoid small peripheral veins due to tissue irritation and necrosis risk.
• Stop the injection if the patient complains of discomfort.
While dilution is not mandatory in a code situation, it may be preferred in some cases:
• Dilution can help reduce the risk of venous irritation.
• For prolonged administration or in non-emergent situations, dilution is often recommended.
Important Notes
• Calcium gluconate is also an option, as calcium chloride is more concentrated and irritating than calcium gluconate, requiring extra caution.
• The use of calcium in cardiac arrest is controversial and not routinely recommended unless there is a specific indication, such as hyperkalemia, hypocalcemia, or calcium channel blocker toxicity.
Kind regards,
Jeff
Tehetena Zarou says
Hi Jeff
just want to double check
is 1 ml of 10 % Calcium chloride equal to 100 mg/ml?
ACLS says
That is correct. 10% calcium chloride is 100 mg/mL. 100 mg of calcium chloride is in 1 mL.
Kind regards,
Jeff
cancelm5 says
wow hey have used this site for while now and never ran into this info tab on the tx of hyper/hypo k.. very easy to follow.. can it be printed?
ACLS says
Yes. You can and should be able to print any of these pages. Kind regards, Jeff
Cecilia says
Helpful information on Hyperkalemia. Have used this site for years and somehow I missed this page. Thank you.
ACLS says
Your welcome! Kind regards, Jeff
Aisha Ali says
very good… very informative. I know most of what has been said..but it still nice to read the detail .. and given in such a succint manner. thank you.
Yolanda Wiid says
What must potassium levels be to be classified as mild, moderate or severe hyperkalemia?
Kind regards
Jeff with admin. says
The severity is divided into mild (5.5-5.9 mmol/L), moderate (6.0-6.4 mmol/L), and severe (>6.5 mmol/L).
Kind regards, Jeff
flieswithsun says
Arrhythmias, Emergent
Indicated for arrhythmias associated with hypocalcemia, hyperkalemia, or hypermagnesemia
Calcium Chloride
500-1000 mg IV over 2-5 minutes
1 g (10 mL) vials of calcium chloride 10% solution in the crash cart = 100mg/ml. Usually the doc just asks for an amp.
Rachel Situmorang says
How to give the D50W with insulin + 10 U insulin in 15-30 minutes? Infusion? Or slow IV bolus?
Jeff with admin. says
D50 + insulin is typically given slow IV push. It can be given over 1 to 2 minutes.
Kind regards,
Jeff
Kelelelo Maphala says
How many times can the 50% dextrose plus insulin solution be given in hyperkalemia of 6 and what are the risks posed when given more than twice?
ACLS says
There’s no strict guideline-mandated limit on how many times insulin-dextrose (often given as 10 units regular insulin with 50 mL of 50% dextrose) can be repeated for hyperkalemia, but clinical evidence shows real dangers accumulate sharply after the first repeat dose, and repeated dosing should be minimized in favor of definitive potassium-removal therapy.
For a potassium level around 6 mEq/L, most protocols classify this as mild-to-moderate hyperkalemia, where insulin-dextrose is one option alongside albuterol, diuretics, or potassium binders, rather than an automatic first-line necessity. If potassium remains elevated or rebounds, which commonly happens 2–4 hours later as the insulin effect wanes, the insulin-dextrose dose can be repeated, but guidelines emphasize this should prompt starting definitive potassium-removal therapy (binders or dialysis) rather than relying on repeated insulin dosing.
Repeated dosing beyond twice is generally discouraged in favor of starting binders, diuretics, or dialysis to achieve lasting potassium clearance, alongside hourly glucose checks for at least 4–6 hours after any dose.
Kind regards,
Jeff
Solomon Wai says
I think one of the major reasons why Calcium Chloride is preferred over Calcium Gluconate in Cardiac Arrest is because Calcium Gluconate needs liver metabolism to extract Calcium whike Calcium Chloride dissociate into Ca++ and Cl- once it hits the plasma.
Maxine21 says
Thanks
Christena says
I see that the AHA guidelines recommend insulin + D50 over 15-30 minutes for the treatment of severe hyperkalemia. It seems that this would require the two components to be mixed in an empty minibag or drawn up in a syringe and put on a pump for infusion? During a code this does not seem practical. Honestly, I have never seen it infused this slowly. I almost always see the insulin pushed, then the D50W pushed, or the reverse (or no D50 if bg is severely elevated). Do you know the rationale for the slow infusion of 15-30 minutes and how this would practically work during a cardiac arrest scenario, especially if you were not planning on giving the dextrose due to severe hyperglycemia?
Thank you,
Christena
Jeff with admin. says
I have always seen it pushed in a code situation. No reason for a slow infusion on a dead person.
The 15-30 min amiodarone infusion that the guidelines address is for a non-coding patient with a tachyarrhythmia that is being treated with amiodarone.
Kind regards,
Jeff
heather says
Is there evidence-based support for calcium chloride over calcium gluconate? I don’t see why gluconate (of course at an equivalent dose) is not an option. Thanks.
Jeff with admin. says
As far as I know, either form of calcium salt would be satisfactory if indicated during cardiopulmonary resuscitation or for the treatment of ionized hypocalcemia due to massive blood transfusion. Here is the reference. Calcium Chloride vs. Calcium Gluconate AHA does only recommend calcium chloride in their resuscitation guidelines.
Kind regards, Jeff
Louise Fowler says
ACLS is now recommending using 100ml of 10% glucose for hypoglycaemia however it is still recommending 50% glucose 10units of insulin for hyperkalaemia. Can we use 250ml of 10% glucose for hyperkalaemia?? Kind Regards
Jeff with admin. says
Toward the bottom of this webpage, your first question is addressed. Regarding your second question, I could not find any information about using 250ml of D10 instead of the 50ml of D50. If D50 was not available, I see no reason why this would be a problem since you would be giving an equal about of dextrose, but the fluid volume would be slightly more.
Kind regards,
Jeff