Ventricular fibrillation (VF) occurs when there are uncoordinated contractions within the ventricles of the heart. The primary cause of VF is hypoxia (lack of oxygen) to the heart muscle, which causes hyperirritability in the cardiac muscle tissue.
As a result, multiple muscle cells within the ventricles simultaneously fire as pacemakers causing a quivering or fibrillation that is ineffective for adequate cardiac output.
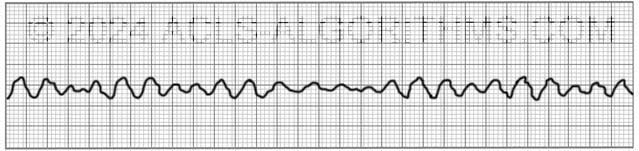
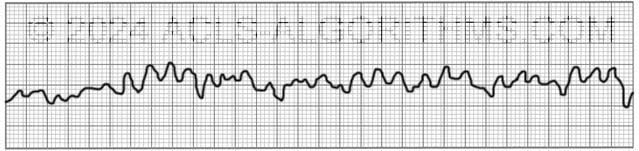
The two images show what ventricular fibrillation will look like on an EKG rhythm strip.
VF can rapidly lead to heart muscle ischemia, and there is a high likelihood that it will deteriorate into asystole.
Ventricular fibrillation is treated using the left branch of the cardiac arrest algorithm. Click below to view the cardiac arrest algorithm diagram. When done click again to close the diagram.
Cardiac Arrest Diagram

Click to view, and click again to close the diagram.
PALS Cardiac Arrest Diagram

Ventricular fibrillation is always pulseless and must be confirmed by EKG or defibrillator monitor. Defibrillation is the treatment of choice and should occur as soon as possible.
The video below shows an example of what ventricular fibrillation will look like when you see it on the defibrillator monitor. Please allow several seconds for the video to load. (7.24mb)
Click for next Rhythm Review: Pulseless Electrical Activity
Top Questions Asked on This Page
-
Q: Why does it say VFib is always pulseless? My thinking is an organized rhythm with no pulse will be PEA, then should be treated as on R branch of the cardiac arrest algorithm.
A: Ventricular fibrillation is not an organized rhythm. It is a chaotic and disorganized rhythm. There is no organization to the rhythm. There are no p-waves and no QRS complexes.
-
Q: Which concentration of Lidocaine is given intravenously in ACLS considering that there is the local anesthetic as well. Is the 2% safe?
A: Typically, lidocaine for IV infusion is mixed 2000 mg lidocaine in 500 ml. This works out to a 4 mg/ml dilution.
Two percent lidocaine is a 20 mg/ml. This 20 mg/ml would need to be diluted to obtain the 4 mg/ml dilution.
You would not want to give 2% lidocaine without diluting to 4 mg/ml. The main reason for dilution is to avoid rapid high plasma concentrations and reduce toxicity risk -
Q: When does the sodium bicarb injection need to be administered and when does the lidocaine IV need to be administered?
A: Here is the AHA position on Sodium Bicarbonate:
“In some special resuscitation situations, such as preexisting metabolic acidosis, hyperkalemia, or tricyclic antidepressant overdose, bicarbonate can be beneficial (see Part 10: Special Circumstances of Resuscitation).
However, routine use of sodium bicarbonate is not recommended for patients in cardiac arrest.”
Here is the AHA position for Lidocaine:
“There is inadequate evidence to support the routine use of lidocaine after cardiac arrest. However, the initiation or continuation of lidocaine may be considered immediately after ROSC from cardiac arrest due to VF/pVT.
Lidocaine may be considered as an alternative to amiodarone for VF/pVT that is unresponsive to CPR, defibrillation, and vasopressor therapy.
carolyncovington says
I cannot see the videos… I am logged in. I registered in November 2016.
thanks
Carolyn covington
Jeff with admin. says
Hi Carolyn,
There are a couple of things that can cause this. You can find a troubleshooting guide in the help area here, or you can give a call to the technical support line and I would be glad to help you trouble shoot the issue. The technical support line is 316-243-7096. Kind regards, Jeff
toni says
what number do you start to shock 100?
Jeff with admin. says
For defibrillation of cardiac arrest the starting shock dose is recommended to be between 100-120 J. Kind regards, Jeff
jade says
I could never take ACLS without you, I would PANIC !!!
Raynald Raynald says
thanks for the nice video, one thing though, so how can you tell for sure the difference between asystole and Vfib that looks like asystole in a monitor or defib monitor
Jeff with admin. says
It can be difficult to differentiate asystole from fine VF. If the the cardiac arrest is sudden and you see immediate asystole after collapse you may suspect fine VF. Asystole means the heart is dead. A heart becoming dead takes time.
The longer cardiac arrest progresses, the more likely the chances that a isoelectric or nearly isoelectric line is asystole. I hope that helps.
Kind regards,
Jeff
Shawnita148 says
That was a great answer! “A heart becoming dead takes time”. It really helps paint the picture and troubleshoot. This program is fantastic!
john philip k. says
ah! what a joy to notice this. so systhematic and easy to understand. thanks.
l just chanced it.
Alergologu says
Hello Jeff!Thank you for this amazing lesson!Could anyone explain to me please the way of epinephrine and amiodarone in the case of cessation of cardiac contractions?How the drugs reach systemic circulation?!
Jeff with admin. says
When you perform uninterrupted high quality chest compressions, you will move the medications to the central circulation. Chest compressions take the place of the cardiac contractions.
Kind regards,
Jeff
sborowiak10 says
After shock number 3 and giving 300mg Amiodarone, are you able to continue giving Epinephrine q 3-5 min between the next 5 cycles of CPR and rhythm check even with the follow up dose of 150 mg coming after the next shock.?
Jeff with admin. says
Yes you can. Epinephrine is basically on its own time table and can be given every 3-5 minutes. Just make sure it is given when chest compressions are being performed. Also make sure that you follow every dose with 20 ml of NS rapid IV push.
Kind regards,
Jeff
Joni R says
Don’t forget to change leads for lead verification if unsure fine V fib vs asystole. If in doubt – shock/defibrillate
zongmei Hanson says
I would like the vedios have voice to explain everything on the diagram because the sounds make me remember better and I could not read it so fast. but I like them anyway. I hope it will help me pass the test this time. thank you
Judith Fusco says
Jeff in your video for V fib it says follow the “pulseless arrest algorithm”. You do mean follow the left side of the Adult Cardiac Arrest Algorithm where it says VF or Pulseless VT: not the PEA (pulseless electrical arrhythmia). I just want to be clear that when you use the words “pulseless arrest algorithm” in your video you do me the left side not the asystole/PEA (both of course are pulseless?
Jeff with admin. says
You are correct. Pulseless arrest algorithm should be stated adult cardiac arrest algorithm left side. This video needs to be updated. Sometimes I find myself calling the cardiac arrest algorithm the pulseless arrest algorithm because it used to be called the pulseless arrest algorithm prior to 2010.
Kind regards,
Jeff
Damilola says
Outstanding! This has really been helpful. Thank you Jeff and Co
Jeff with admin. says
I’m that that you have found the site helpful. Kind regards, Jeff
Avani says
This is a very useful site.Thanks for all your help.Just wanted to ask We have an AED instead of a DEFIBRILLATOR.Can I use AED instead of a Defibrillator for shock in PULSELESS VT/VF.
Jeff with admin. says
Yes you can. The AED will just slow your process down.
Kind regards,
Jeff
Fiona says
I was stressed about taking ACLS for the first time…………thankyou so much for sharing this wonderful site………..you made it so much less stressful.
Jeff with admin. says
I’m so glad that the site has been helpful for you. Kind regards, Jeff
Nancy says
I love your site. one question on exam was “What would be your very first action if you have pulseless V.T.
The answer was defib. first and yet the algorithm says to start C.P.R. first.
Thank you Nancy
Jeff with admin. says
If the patient is attached to the defibrillator then the first action would be defibrillation. If the defibrillator is not attached then you would start CPR. Was this not made clear in the question?
Kind regards,
Jeff
patrickfanelli says
I have the AHA provider manual and it puts me to sleep! I have just started using you website for 10 min and I am already hooked! This will probably be the best 16.95 I ever spent! I am a Wildland Fire Fighter in FL. So I do not run any medical calls. But I am also a Paramedic and this site is going to keep my skills up to date and prepare me for my renewal . Good job with this site!
Thanks!
Jeff with admin. says
I’m so glad that the site is helpful. Kind regards, Jeff
Stu the Medic says
THANK YOU to whoever set this website up and keep it running smoothly!!! It is so awesome, so easy to learn, and entertaining as well: love the drama music during rhythm videos. May God bless you and give you many donations for your efforts!
Jeff with admin. says
Thanks for the complement. We will do our best to keep the site as educational, entertaining, and user friendly as possible. Kind regards, Jeff
Marcella says
Just started! This is awesome! I’ve passed courses in the past, but this time I’m understanding. Thank you!