Second degree heart block Type 2, which is also called Mobitz II or Hay, is a disease of the electrical conduction system of the heart. Second-degree AV block (Type 2) is almost always a disease of the distal conduction system located in the ventricular portion of the myocardium.
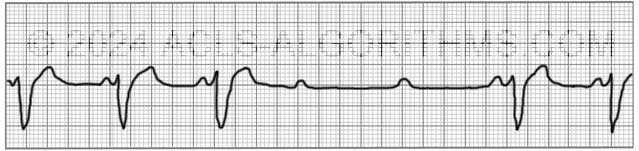
This rhythm can be recognized by the following characteristics:
- non-conducted p-waves (electrical impulse conducts through the AV node but complete conduction through the ventricles is blocked, thus no QRS)
- P-waves are not preceded by PR prolongation as with second-degree AV block (Type 1)
- fixed PR interval
- The QRS complex will likely be wide
Click here to see why.
The QRS on an ECG will most likely be wide because the block occurs in the His bundle or bundle branches and conduction through the ventricles is slowed. This slowing of conduction appears as a wide QRS complex on the ECG.

Second-degree heart block type 2 is usually caused by structural damage to the conduction system of the heart. Causes of the structural damage to the conduction system include the following:
Causes:
- Myocardial infarction that damages the conduction system
- Idiopathic fibrosis
- Cardiac surgery
- Infections and inflammatory conditions
- Hyperkalemia
- Autoimmune diseases affecting the heart
Second-degree AV block (Type 2) should be treated with immediate transcutaneous pacing or transvenous pacing because there is risk that electrical impulses will not be able to reach the ventricles and produce ventricular contraction.
Second-degree AV block (Type 2) is clinically significant because this rhythm can rapidly progress to complete heart block.
Atropine may be attempted if immediate TCP is not available or time is needed to initiate TCP. Atropine should not be relied upon and in the case of myocardial ischemia it should be avoided.
Below is a short video which will help you quickly identify second-degree heart block type 2 on a monitor. Please allow several seconds for the video to load. (2.65 mb)
Click for next Rhythm Review:
Complete Heart Block (3rd Degree Block)
Top Questions Asked On This Page
-
Q: The video says “sometimes has wide QRS.” What else would you see with 2nd-degree if the block is occurring in the bundled His? I have seen the portrayed rhythm many times and was not sure what it was.
A: For 2nd-degree block type II you will see:
non-conducted p-waves (electrical impulse conducts through the AV node, but complete conduction through the ventricles is blocked, thus no QRS)
P-waves are not preceded by PR prolongation as with second-degree AV block (Type 1)
fixed PR interval -
Q: Having trouble differentiating between Mobitz II and third-degree block.
A: The main difference is this:
Mobitz II: There will be a P-wave with every QRS. There may not always be a QRS complex with every p-wave. The rate will usually be regular. Also, the PR interval will be regular.
3rd Degree Block: There may not be a p-wave with each QRS, and the PR interval will not be the same with each PQRS.
These videos may help you.
They are kind of hard to hear, but the content is good. -
Q: Your video says pace right away for 2nd degree? TCP should only take place if the patient is symptomatic or showing signs of inadequate perfusion? Correct?
A: Correct. If the patient is unstable which is defined as “showing signs of poor perfusion.”
James jones says
What if the patient is asymptomatic and it was picked up on routine testing in the ED when the patient attended for another complaint. Does it still need management?
Jeff with admin. says
The patient would definitely need to be evaluated and may need management depending on the situation. This does happen and should not be ignored.
Kind regards,
Jeff
Leslie says
Thank you so much for the information on heart blocks! You unraveled the mystery for me.
Leslie
jbgenobisa says
Hi Jeff,
With symptomatic Bradycardia when do we decide among Atropine, epinephrine or dopamine should be used?
Jeff with admin. says
Epinephrine and dopamine are used as an alternative to transcutaneous pacing. These two medications would be used for symptomatic would be used for symptomatic Bradycardia with poor perfusion.
Generally speaking, atropine would be your initial choice for treating any type of symptomatic bradycardia.
Once you have advanced to the point of having a patient with compromised perfusion you would want to rapidly moved to the use of epinephrine or dopamine or transcutaneous pacing.
Kind regards,
Jeff
Faten says
why are the QRS complexes inverted?
Jeff with admin. says
In the rhythm strip that you referenced, the QRS complex inversion has to do with the lead that is being monitored. The direction of the electrical discharge is what dictates whether the QRS complex is deflected above or below the isoelectric line.
Kind regards,
Jeff
Katie says
My 11 month old son has 2 degree heart block (type II).
Haboobeker Naimee says
thats terrible does it it look like the one on the EKG or in like in the Nancy Caroline Emergency care on the streets textbooks?
Laura B says
I would love to know about how the 2nd degree Av Block presents itself symptom wise.
Jeff with admin. says
The symptoms of 2nd degree block would normally be association with the symptoms of bradycardia which would include symptoms caused by poor blood perfusion.
Some symptoms would include chest pain/discomfort, decreased blood pressure, restlessness, confusion, cool extremities, pallor or cyanosis of extremities, diminished or absent peripheral pulses, slow capillary refill.
Kind regards,
Jeff
Dee Dee Dirks says
Looking at Second-Degree AV block type I vs type II- how do you distinguish the difference when trying to identify the rhythm ? Third-degree AV block is clear but I’m having difficulty seeing the difference between the 2 types of Second-degree blocks
Btw, your program has been super helpful!! Thank you!
Jeff with admin. says
The easiest way to differentiate is this:
2nd block type I Can be recognized by observing and increasing PR interval with an eventual drop in a QRS complex. The PR interval will go longer, longer, longer, drop.
2nd degree block type II can be recognized by observing a missing QRS complex. Unlike 2nd block type I, the PR interval’s will all be the same.
Kind regards,
Jeff
tecintron says
Hi Jeff!
I am a new nurse and I am curious as to why the QRS points are pointing downward (probably a stupid question).
The music reminds me of Mission Impossible!! I love it!
Jeff with admin. says
This is a good question. In the video, the QRS complexes are “pointing down” (negatively deflected) because this rhythm is being observed from a lead in which the electricity is moving away from the lead being observed. There are 12 leads that can be read on an ECG and some of them are normally negatively deflected.
Basically, if the lead that you are looking is negatively deflected the electricity is moving away from the lead. If the lead that you are looking at is positively deflected the electricity is moving toward the lead.
This stuff can get a bit technical and is way beyond basic ACLS. If you would like understand more about ECG axis and 12 lead interpretation, here is a ECG axis.
Here is a link to a Normal 12 lead wavesof that all of the normal leads look like.
For the beginner, the lead that is the “easiest” and most common to look at is Lead II, but all of the rhythms that are learned in ACLS can be easily interpreted no matter what lead you are looking at.
Kind regards,
Jeff
brendabikes says
2nd recert next month. 2nd time using your site. Thank you so much. My only suggestion would be to make the images larger (the defib monitor) as well as some of the writing. I find myself squinting and sitting close to the computer.
Jeff with admin. says
I’m so glad that you have found the site helpful. The videos found on the ACLS rhythm interpretation section of the knowledge base were created using software that was formatted for standard definition. They are in the process of being edited to improve the screen quality. They will eventually (within the next 6 months) be the same improved quality as found in the megacode series videos and the rapid rhythm ID videos.
Kind regards,
Jeff
vicki says
In all the heart blocks is seems to me that the p to p interval is consistent. Or in old school terminology they “walk off’.This is not mentioned regarding Mobitz type 2, am I correct or incorrect?
Jeff with admin. says
You are correct. For the most part, all blocks will have a consistent p to p interval.
Kind regards,
Jeff
Mary Benson says
Thank you Jeff for this wonderful site and explanations. Love the video examples.
Very helpful.
After 30 yrs. of being a PA/FNP I am studying for boards to recertify.
Thank you,
Mary
Jeff with admin. says
I’m so glad that the site is helping. Kind regards, Jeff
Jbailey777 says
Hi Jeff,
It says in the red box above “Atropine may be attempted if immediate TCP is not available or time is needed to initiate TCP. Atropine should not be relied upon and in the case of myocardial ischemia it should be avoided.” But on page 166 in the manual, it says in bold that “Atropine Sulfate will not be effective for infranodal (Mobitz type II) block.”
So regardless if you don’t have immediate access to TCP, don’t try Atropine?
What do you think?
Thanks!
JB
Jeff with admin. says
Atropine may be used and can be effective with any type of sinus bradycardia. It can be effective and should be attempted if possible. With Mobitz II and 3rd degree block at worst, it won’t work. It won’t hurt to try.
If there is a possibility of ischemia then atropine should be used with caution because it can worsen ischemia.
Atropine can be effective for increase heart rate and can improve symptoms that are being caused by the low heart rate. I would use atropine if time and the situation permits.
Kind regards,
Jeff
faustina says
I cannot watch the video there was no picture of video to load
Jeff with admin. says
If you are having this problem on all of the videos, you may need to update your flash player. You can find out how to do that here: Video Help
If you can see some of the videos then this problem is most likely related to the WiFi getting hung up. The easiest way to solve the problem is to restart your computer. You may also want to reset your WiFi router if the computer restart does not solve the problem.
All of the videos do seem to be working fine of the server side.
Kind regards,
Jeff
sweeneyzach34 says
Is the reason for atropine being avoided in cardiac ischemia due to the fact you want to keep oxygen demand low for the heart? And if thats the case but your patient is still unstable after nitro and other interventions what is the best option?
Jeff with admin. says
Correct. Atropine with increase the heart rate significantly and could potentially worsen ischemia. Your best option in this situation would be to use TCP and pace at as low a heart rate as possible that will minimize symptoms while you get the patient to PCI.
Kind regards,
Jeff
Gretzel Mae Deang says
hello.. i would likely to know the difference between mobitz2 type1 and mobitz2 type2 in an ecg example? thank u
Jeff with admin. says
You terminology is a bit off. There is Mobitz 1 and then there is Mobitz 2
Mobitz 1 = 2nd degree type 1 This explains Mobitz 1.
Mobitz 2 = 2nd degree type 2 (The page that you are on right now explains Mobitz 2.)
Kind regards,
Jeff
wgres@hotmail.com says
In the 2010 up date it said initial treatment of bradycardia is Atropine.
Jeff with admin. says
“In the 2010 up date it said initial treatment of bradycardia is Atropine.”
On page 111 of the AHA Provider Manual it states:
“Atropine administration should not delay the implementation of external pacing for patients with poor perfusion.”
Also on page 111 it states:
“Do not rely on atropine in Mobitz Type II and also 3rd degree block or in patients with third-degree AV block with a new wide QRS complex.”
The above would be the main reason for skipping over the atropine and going straight to TCP if it is ready for use.
Kind regards,
Jeff