There are several other tachycardia rhythms that can be seen with both stable and unstable tachycardia. These rhythms include monomorphic ventricular tachycardia and polymorphic ventricular tachycardia both of which are wide-complex tachycardias.
Wide complex tachycardias are defined as a QRS of ≥ 0.12 second. Expert consultation should be considered with these rhythms.
These wide-complex tachycardias are the most common forms of tachycardia that will deteriorate to ventricular fibrillation.
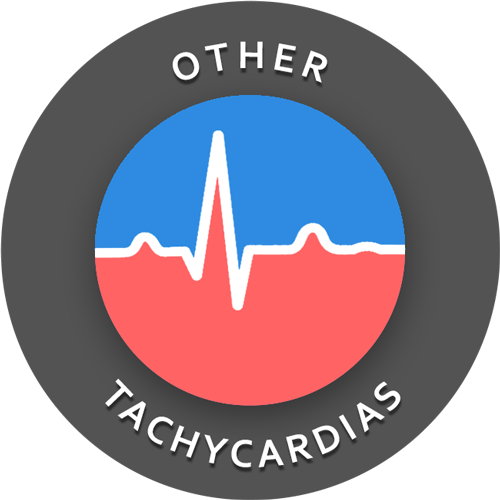
Monomorphic Ventricular Tachycardia
With monomorphic VT all of the QRS waves will be symmetrical. Each ventricular impulse is being generated from the same place in the ventricles thus all of the QRS waves look the same.
Treatment of monomorphic VT is dependent upon whether the patient is stable or unstable. Expert consultation is always advised, and if unstable, the ACLS tachycardia algorithm should be followed.
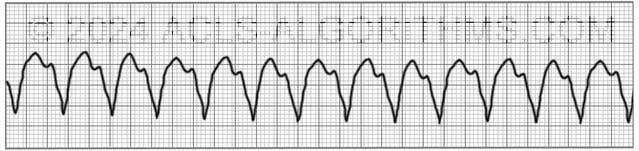
Polymorphic Ventricular Tachycardia
With polymorphic ventricular tachycardia, the QRS waves will not be symmetrical. This is because each ventricular impulse can be generated from a different location. On the rhythm strip, the QRS might be somewhat taller or wider.
One commonly seen type of polymorphic ventricular tachycardia is torsades de pointes. Torsades and other polymorphic VT are advanced rhythms which require additional expertise and expert consultation is advised.
If polymorphic VT is stable the ACLS tachycardia algorithm should be used to treat the patient. Unstable polymorphic ventricular tachycardia is treated with unsynchronized shocks (defibrillation). Defibrillation is used because synchronization is not possible.
These wide complex tachycardias tend to originate in the ventricles rather than like a normal rhythm which originates in the atria.
Top Questions Asked On This Page
-
Q: What are the doses for synchronized cardioversion?
A: Here are the cardioversion voltage doses:- Narrow regular: 50-100 J
- Narrow irregular: 120-200 J biphasic or 200 J monophasic
- Wide regular: 100 J
- Wide irregular: defibrillation dose (not synchronized)”
All of this information is covered on the tachycardia algorithm page.
-
Q: Is it necessary to memorize the doses listed above?
A: It is necessary to understand the concepts and be familiar with the shock dosages.
The repetition that is built into the website is designed to help you become very familiar with all of the concepts and use them in emergencies. -
Q: What sort of a pulse would you be feeling with a polymorphic VT?
A: You may feel a weak pulse or a strong pulse depending on how long the polymorphic VT has been going on. One thing is for sure….You won’t be feeling a pulse for very long if this rhythm continues.
fahmawi mhmod says
I think it would be easy to say trade by wide copmlex tachecardia protocol. If there any pulss
KAS says
When a patient goes into monomorphic v-tach, does the rhythm need to look identical in all leads or can it look different? Ex. Lead II: QRS has negative deflection Lead VI: QRS is up right, They both marge out to have a rate of 164, P wave is not visible but may be hidden. so if its not considered monomorphic v-tach, what are the other possible diagnosis for this?
Jeff with admin. says
Other possible diagnosis would be some type of tachycardia with an underlying block that causes the QRS complex to be wide. This type of rhythm can look very similar to VT and is probably the most common rhythm that is confused with VT.
Kind regards,
Jeff
Sophiels85 says
Hi!
What would be the appropriate initial energy level for defibrillation of an unstable pt (w/ a pulse) with a wide & irregular tachycardia?
Would it be 120-200J on a biphasic defibrillator as in the pulseless arrest algorithm?
Thank you!
Jeff with admin. says
Because the rhythm is wide complex and irregular you most likely will not be able to sync the defibrillator. In this case, you would perform defibrillation (NOT synchronized). Starting dose would be 122-200 J. You would increase incrementally and stepwise fashion after this. 120-200-300-360.
Kind regards,
Jeff
Rmbutler says
Should you use mag sulfate immediately after shock if not converted in polymorphic VT? Without getting labs? Or use amiodarone? I am confused. What is the dose of mag sulfate if you give it and is there a limit?
Jeff with admin. says
If a patient is in polymorphic VT, you would begin to consider magnesium sulfate after the first shock. It is ok to give the Mag. Sulfate for polymorphic VT if hypomagnesaemia is suspected. Amiodarone can also be administered.
Give Magnesium sulfate 1 to 2 g is diluted in 100 mL D5W and administered over 1 to 2 minutes. Rapid administration of magnesium may cause clinically significant hypotension or asystole and should be avoided.
This is a quote from AHA website:
“Anecdotal experience suggests that magnesium may be an effective treatment for antiarrhythmic drug-induced torsades de pointes even in the absence of magnesium deficiency. A variety of dosing regimens for magnesium sulfate have been described. Magnesium may be administered as a loading dose of 1 to 2 g (8 to 16 mEq), mixed in 50 to 100 mL D5W, given over 5 to 60 minutes, followed by an infusion of 0.5 to 1.0 g (4 to 8 mEq) per hour. The rate and duration of the infusion should be determined by the clinical situation. The routine prophylactic administration of magnesium in patients with AMI is no longer recommended. Magnesium is not recommended in cardiac arrest except when arrhythmias are suspected to be caused by magnesium deficiency or when the monitor displays torsades de pointes.”
http://circ.ahajournals.org/content/102/suppl_1/I-112.full
Kind regards,
Jeff
jeremey says
The AHA’s supplementary material states that polymorphic VT will rapidly deteriorate to pulseless VT or VF. How likely is a patient to present as “stable” and if they are stable should we only adminster 150 mg of amiodarone as opposed to the 300 mg used in VF and VT ?
Jeff with admin. says
It is unlikely that a patient in polymorphic VT will be stable. In the case that they are stable, you would follow the tachycardia antiarrhythmic protocol which calls for 150mg IV over 10 minutes and this may be repeated every 10 minutes as needed. An infusion per protocol may also be considered.
Kind regards,
Jeff
retiringsoon says
Hi Jeff,
How would we treat a patient with SVT, pulseless, unresponsive.
thanks for your response.
Jeff with admin. says
You are not likely to see an unresponsive patient with SVT that is pulseless. SVT will degenerate to VF or asystole before a patient is unresponsive and pulseless.
Now let’s address this issue. You will likely know how the patient had progressed to get to this point. If the patient had been unstable with SVT prior to unresponsiveness, they probably should have been cardioverted.
However if you did not know the history, this would most likely be treated as PEA. So CPR, epinephrine and addressing the cause of the PEA (H’s and T’s) would be indicated.
If treated as PEA, after a cycle of CPR if a cause cannot be identified and dealt with, it may be prudent to attempt cardioversion. There is the possibility of the pulse being to weak to palpate. A cardioversion attempt will not hurt, but it may help if this is truly SVT.
After the cardioversion, you would immediately begin CPR and continue with the PEA asystole algorithm.
Hope this makes sense.
Kind regards,
Jeff
Lee says
Good day Sir
If a patient goes into cardiac arrest and they have any form of polymorphic Vtach (including Torades) should I defibrillate like I would for pulseless monomorphic Vtach of V-fib?
I ask as I can do manual defibrillation but I can’t do cardio version or give ACLS drugs at my current qualification.
Also, sitting in the back of an ambulance, I am probably unlikely to sit and work out what type of polymorphic Vtach it is.
Can defibrillating a pulseless torsades cause a decrease in chance of a successful resus?
Thank you in advance
Jeff with admin. says
First question answered:
Cardiac arrest is a state of pulselessness. If a patient is in cardiac arrest and has any type of VT whether it is Torsades, monomorphic VT, or any other polymorphic VT, defibrillation should be used. These are all treated the same. Except, you would possibly use Magnesium if you are dealing with Torsades de Pointes.
Second question answered:
I have never read anything to support that. A pulseless torsades means the patient has no blood flow, so CPR and defibrillation would be the treatment of choice.”
Kind regards,
Jeff
Vivian says
Happy to join this site again for my ACLS recert.. Do you have an app for your site Jeff? I want it on my phone homescreen if available, Thx so much.
Jeff with admin. says
I don’t have an app, but you can easily create a icon link on the home screen of your phone.
If you have i-phone do this. Browse to the home page of the website in Safari. At the bottom of the screen, you will see a box with an up arrow in it. When you touch this, you will see some options. One of them is “Add to home screen.” When you touch this, it will add an icon for the website to the home screen of your phone.
If you using android, open google chrome and navigate to the home page of the website. Then touch your menu button (probably in the top right. You should then see a tab that says “add to home screen.” Touch this and it will add an icon for the website to your home screen.
If this does not work, google search “your phone type, how to add website to home screen.”
Kind regards,
Jeff
Guyton says
Polymorphic VT may be stable or unstable (not in arrest). If unstable, desfibrilation is required. Is it necessary CPR like VF??
Thanks
Jeff with admin. says
CPR would be required if the patient becomes pulseless. Unsynchronized defibrillation would be the most important intervention for polymorphic ventricular tachycardia that is unstable.
Kind regards,
Jeff
Guyton says
Thanks Jeff!!
So is it not necessary CPR after desfibrilation if the patient has signs of spontaneous circulation?
May you tell me any reference about this topic?
Best regards,
Guyton
Jeff with admin. says
No. If you have performed unsynchronized defibrillation on a pulseless patient who is in VF or VT you would then perform 5 cycles of CPR before performing a rhythm or pulse check.
Kind regards,
Jeff
Matt says
Unsynchronized shock for unstable polymorphic VT even with a pulse?
Jeff with admin. says
Yes, most of the time polymorphic VT will need to be shock with unsynchronized shocks. This is because the defibrillator will not be able to sync with the rhythm due to the non-regular nature of polymorphic VT.
Kind regards,
Jeff
Blonde4fun says
After going through the aha rhythms, I got a little confused. It seems like they are implying that polymorphic VT is Torsades ( I know that it is a type of VT). How do you distinguish between polymorphic VT that twist and PVT that is just extremely fast?
Thanks so much. You guys and the entire website are AWESOME!
Jeff with admin. says
Torsades is a type of polymorphic VT. With this type of VT, the electrical firing of the heart is following a specific patter in the heart which is kind of like a circle around the ventricle. When this circular pattern of electrical firing is seen on an ECG it looks like this.
Other types of polymorphic VT do not have a regular patter of firing but are random and varied throughout the ventricle. This type of polymorphic VT will look something like this.
For Torsades to be diagnosed, the patient has to have evidence of both PVT and QT prolongation. Without these two things you would consider the rhythm regular polymorphic VT and treat it as such.
Kind Regards,
Jeff
christinala says
If you give magnesium and calcium for Torsades, does the calcium decrease the effect of the magnesium?
Jeff with admin. says
Hard to say. The reason you would give calcium would be for suspected hypocalcemia and magnesium for low magnesium. No research that I know of has looked at this and I see no reference in any of my ACLS references.
Kind regards,
Chris
Christopher Kaphaem says
Magnesium and calcium work together at precise ratios to ensure proper heart function, and magnesium can affect calcium levels much more than the reverse. Magnesium competes with calcium for absorption and can cause a calcium deficiency if calcium levels are already low. Hope this helps.
Jeff with admin. says
Thanks for sharing this Christopher. Kind regards, Jeff
Julia says
Hi Jeff,
This site is wonderful!
I was wondering, if the torsade the points persists even after the Mg solfate and the patient is unstable and you need to defibrillate him/her, how many Joule would you use? 360 J?
Thank you!
Jeff with admin. says
It would depend on the size of the patient:
Small patient: 120 then 200 then 300 then 360
Large patient: 200 then 300 then 360
With each subsequent dose, the heart becomes a little more refractory to the electrical shock so you must make sure and increase the shock dose by at least 50 joules.
Kind regards,
Jeff
SP07 says
Regarding the term ‘VT’ – how do you differentiate VT rhythm and polymorphic VT rhythm when looking for a few seconds on the monitor?
Jeff with admin. says
Actually VT is a general term. Polymorphic VT and Monomorphic VT would both fall in the category of VT and in particular will be seen with pulseless VT. If you look at this link it explains the difference and gives a couple of rhythm strip examples.
Kind regards,
Jeff
tslater says
Jeff,
I understand that Mg is the drug of choice in polymorphic v-tach if the q-t interval is prolonged.
I do not see a q-t interval. Do you need to see the rhythm prior to the tachy-dysrrhymia?
Chris with admin. says
Yes. you need to see the rhythm prior to torsades. If a patient is on telemetry, the QT interval should be be measured at least once per shift. The QT interval is dependent on the heart rate and must correct based on the heart rate using the following formula.
1. Bazett HC. An analysis of the time relationships of electrocardiograms. Heart. 1920;7:355-70.
RRInterval = 60 / HeartRate
QTICorrected = QTInterval / sqr(RRInterval)
Kind regards,
Chris Jack
Jonathan says
2 questions:
1) What sort of a pulse would you be feeling with a polymorphic vt ?
2) Which tachycardias would you use a amioderone infusion?
Thanks
Jeff with admin. says
1.)You may feel a weak pulse or a strong pulse depending on how long the polymorphic VT has been going on. One thing is for sure….You won’t be feeling a pulse for very long if this rhythm continues.
2.)You will use the amiodarone for pulseless VT/VF, and other recurrent hemodynamically unstable VT (monomorphic or polymorphic); probably won’t use it on narrow complex tachycardias.
Kind regards,
Jeff
jonathanjung says
When would see torsades? with pulse w/o pulse . Magnesium would be your drug of choice if QT was prolonged. How would you give Mg with pulse w/o pulse? (dose, time and dilution) Thanks
Jeff with admin. says
Common causes for torsades de pointes include diarrhea, hypomagnesemia and hypokalemia. It is commonly seen in malnourished individuals and chronic alcoholics.
Correct, magnesium would be your drug of choice if the QT is prolonged.
For torsades de pointes with cardiac arrest, give 1 to 2 g of MgSO4 IV push over 5 to 20 minutes. If torsades de pointes is intermittent and not associated with arrest, administer the magnesium over 5 to 60 minutes IV. If seizures are present, give 2 g IV MgSO4 over 10 minutes. Administration of calcium is usually appropriate because most patients with hypomagnesemia are also hypocalcemic.
Kind regards,
Jeff
Cmhallrn says
With a pt in polymorphic v tach who is stable and experiencing long periods of this ( 12 seconds and longer) who states he “feels ok” what is the best first and second course of action?
Jeff with admin. says
1. Get a crash cart next to him with the defibrillator attached.
2. Consult a cardiologist ASAP
(ECG, O2, Labs esp. metabolic panel, and all of the routine stuff would be good also)
Kind regards,
Jeff