There are several other tachycardia rhythms that can be seen with both stable and unstable tachycardia. These rhythms include monomorphic ventricular tachycardia and polymorphic ventricular tachycardia both of which are wide-complex tachycardias.
Wide complex tachycardias are defined as a QRS of ≥ 0.12 second. Expert consultation should be considered with these rhythms.
These wide-complex tachycardias are the most common forms of tachycardia that will deteriorate to ventricular fibrillation.
Monomorphic Ventricular Tachycardia
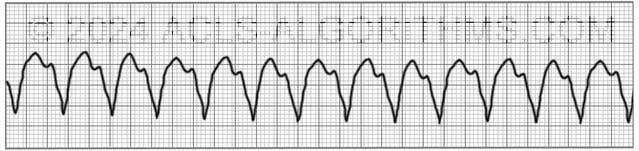
With monomorphic VT all of the QRS waves will be symmetrical. Each ventricular impulse is being generated from the same place in the ventricles thus all of the QRS waves look the same.
Treatment of monomorphic VT is dependent upon whether the patient is stable or unstable. Expert consultation is always advised, and if unstable, the ACLS tachycardia algorithm should be followed.
Polymorphic Ventricular Tachycardia
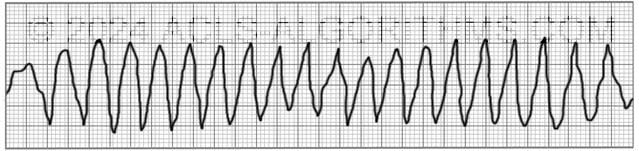
With polymorphic ventricular tachycardia, the QRS waves will not be symmetrical. This is because each ventricular impulse can be generated from a different location. On the rhythm strip, the QRS might be somewhat taller or wider.
One commonly seen type of polymorphic ventricular tachycardia is torsades de pointes. Torsades and other polymorphic VT are advanced rhythms which require additional expertise and expert consultation is advised.
If polymorphic VT is stable the ACLS tachycardia algorithm should be used to treat the patient. Unstable polymorphic ventricular tachycardia is treated with unsynchronized shocks (defibrillation). Defibrillation is used because synchronization is not possible.
These wide complex tachycardias tend to originate in the ventricles rather than like a normal rhythm which originates in the atria.
Top Questions Asked On This Page
-
Q: What are the doses for synchronized cardioversion?
A: Here are the cardioversion voltage doses:- Narrow regular: 50-100 J
- Narrow irregular: 120-200 J biphasic or 200 J monophasic
- Wide regular: 100 J
- Wide irregular: defibrillation dose (not synchronized)”
All of this information is covered on the tachycardia algorithm page.
-
Q: Is it necessary to memorize the doses listed above?
A: It is necessary to understand the concepts and be familiar with the shock dosages.
The repetition that is built into the website is designed to help you become very familiar with all of the concepts and use them in emergencies. -
Q: What sort of a pulse would you be feeling with a polymorphic VT?
A: You may feel a weak pulse or a strong pulse depending on how long the polymorphic VT has been going on. One thing is for sure….You won’t be feeling a pulse for very long if this rhythm continues.
nick says
Pulseless v tach and Polymorphic Ventricular Tachycardia look a lot alike to me. Is the main difference just one has a pulse and the other doesn’t? Are there other “things” I can look for to help me differentiate? Thanks
Jeff with admin. says
You cannot compare pulseless VT with polymorphic VT. This is because any VT can have a pulse or be pulseless. Polymorphic VT can be with a pulse or without a pulse.
You can compare Polymorphic VT with Monomorphic VT. Polymorphic VT will have QRS complexes that WILL NOT all look uniform. This is because the electrical impulse being generated in the ventricles is not generated from the same location every time.
Monomorphic VT on the other hand has the electrical impulse generated every time from the same location in the ventricles and therefore, the QRS complexes will look uniform and identical.
I hope that makes sense.
Kind regards,
Jeff
ammar says
if the patient has pulsless monomorphic VT , the treatment is defibrillator (unsynchronized D.C shock 200 joles ) just like the treatment of pulsless polymorphic VT right ?
Jeff with admin. says
That is correct. The treatment would be to given unsynchronized shock of 120-200 J.
Kind regards,
Jeff
a says
can we decide that this patient has unstable vt by by mental confusion or headlightness only ?
and if the systole BP is 90 can we consider this is unstable vt or we consider instability if the systole is less than 90 ?
Jeff with admin. says
There is room for making judgement calls with these signs and symptoms and nothing is written in stone. Generally speaking a SBP less than 90 with other signs like lightheadedness or LOC changes would be a signs that the patient is unstable. When a patient is unstable, you will likely have several symptoms.
If a patient has only lightheadedness, this would not always be an indicator of an unstable condition. Lightheadedness can will typically be accompanied by other signs. Low BP being one of them. Chest pain and LOC changes being others.
Kind regards,
Jeff
Monica says
I’m a little confused as to when you would give Amiodarone 150 mg over 10 minutes. Is it used for stable monomorphic VT and stable polymorphic VT? Or just stable monomorphic VT?
Jeff with admin. says
The Amiodarone infusion 150 mg over 10 minutes is for use within the tachycardia algorithm. It can be used for both stable monomorphic and polymorphic VT. An amiodarone infusion like this does have risks and should be carried out with the consultation of a cardiologist particularly when considering it’s use with polymorphic VT.
Kind regards,
Jeff
bmuhr11 says
For ems purposes, if the patient presents as “unstable” w/ vtach and a pulse would you still consider synch cardioversion if monophormic? Or would you immediately consider procainamide or amiodarone infusion?
Jeff with admin. says
For EMS purposes, you would want to follow the procedure your EMS has established in the standards of practice. Some strictly follow the AHA guidelines, but there are some that slightly deviate from the AHA guidelines. Strictly following the AHA guidelines the answer would be perform cardioversion for unstable VT. This is what I would say would be the best option. Cardioversion is simple and extremely effective. Any antiarrhythmic medication is going to come with side effects you may have to deal with.
Hope that makes sense.
Kind regards,
Jeff
abosuyonov says
Hello Jeff.
1)For stable Aflutter and atrial tachycardia , may one use Adenosine before BB/ CCB?
2)Are vagal Maneuvers also indicated for Afib, atrial flutter and atrial tachycardia or only for SVT?
Jeff with admin. says
Here is a quote:
Reference: JEMS
Kind regards, Jeff
DR.WAHDAN says
if adenosin is absolutely C/I in AF/A.FLUTTER it block AVN conduction,so vagal manouvers are C/I because they act in the same way.
BridNiF says
‘With monomorphic VT all of the QRS waves will be symmetrical.’
Should this be identical rather than symmetrical … the waves look the same but aren’t made up of exactly similar parts facing each other or around an axis?
Thanks, B
Jeff with admin. says
The QRS complexes will not always be identical. Due to the variation that comes with breathing and other biological factors, the QRS complexes will look symmetrical but not identical. You might see slight variations from beat to beat, but generally speaking the QRS complexes will look the same.
Kind regards,
Jeff
Nadia says
I see no video at all posted for mono and poly VT.
Thanks
Nadia
Jeff with admin. says
The monomorphic and polymorphic ventricular tachycardia page does not have a video posted with it at this time.
Kind regards,
Jeff
ammar says
if the patient has tachyarrhythmia (svt , af , flutter ,or vt ) and systole is 85 ….there is pulse ….we performed cardioversion (synchronized) …if this cardioversion has failed and we used the highest energy (200 jule ) what the next step ?
Jeff with admin. says
Most likely the next step would be to initiate IV antiarrhythmic therapy.
Secondary shocks at the highest shock dose would also be indicated. There is a high percentage of conversion when synchronize cardioversion is use. It is unlikely that you would even need to reach the highest energy level.
Kind regards,
Jeff
viviana7 says
the videos did not play at all. the written information was very helpful. I was disappointed I did not was able to play the videos for review. It would have make it better.
Jeff with admin. says
I checked on the videos and everything seems to be working from the server-side. You may need to update your flash player. This is the most common problem when customers have difficulty viewing the videos.
If you need assistance with this you can call the technical support line 316-243-7096
Kind regards,
Jeff
shirley says
i have been a nurse for 35+ yrs. live in south-eastern ky. and we use soa or sob
samo says
Hi Jeff
Can I ask the reason why do we give Magnesium in cases of self limiting SVT, torsades et.al.
Does it relaxes the heart and settle down the irregular rhythm.
Thank you
Jeff with admin. says
Magnesium is normally indicated for torsades. This is the most common rhythm that is seen with hypomagnesaemia. Magnesium does tend to affect muscle relaxation through direct action on cell membranes. Mg2+ ions close certain types of calcium channels which conduct a positively charged calcium ions into neurons. With an excess of magnesium, more channels will be blocked and nerve cells will have less activity.
Kind regards,
Jeff
Willy says
And most often the patient with torsades arrythmia with history of alcoholism or malnutrition.
tetratetra says
SOA really? How about some Help!
Jeff with admin. says
SOA stands for “short of air.” This is basically the same as SOB “Short of breath.” Depending on where you living in the US will depend on what will be used. Here in the central US, both are used interchangeably. Kind regards, Jeff
Teresa S says
I live in central USA – have never heard SOA. And SOB generally is not used either – due to publics understanding of it. Best not to use initials without defining them first.
Rachel says
I live in the midwest and I have heard of both SOA and SOB and I am just a student. Teresa are you even in the healthcare field???? It is common medical knowledge, similar to HR, HPI, etc…
Angela says
Dear Rachel,
You should be kinder to your soon to be peers in the field. I have been practicing for 12 years and when I was in school they let it be known that SOB stood for shortness of breath, however they also taught us that we NEVER write it on a chart! It was upsetting patients who saw the appreciation and thought providers were calling them names or being derogatory towards them. Not all patients are going to have a high education level, but SOB in a derogatory way is well known across all socioeconomic backgrounds. Dyspnea is the preferred term here in the Midwest. We do not use SOB or SOA.
Kellie Cosimano says
I live on the west coast and worked 30+years in the health care field (paramedic and now RN). I also have never heard SOA used in any setting. Perhaps it is a mid west thing?
Ian G Garcia says
West coast here and 1.2 years as a new-ish ICU RN. Yes we do learn SOB in school, and yes we do understand the public’s first understanding of that abbreviation , hence we keep it between ourselves and don’t tell patient’s families that their loved one the abbreviated term! Never heard SOA until this website, but hey, they preach to us in new grad programs to be flexible. So it goes!
ckaphaem says
I’ve been in healthcare for almost 15 years in the midwest and have never heard of SOA.
kathymanelis says
I have been an RN for 33 years, cardiac for 20 of those years, and ICU for the last 13+ years. I have worked in the midwest in multiple hospitals and in New England in multiple hospitals. I have never once heard the term SOA. I have heard the term SOB used throughout health care but only abbreviated in notes among healthcare professionals, never with patients’ families. Of note, before we went to EMR, I did see it in the MD Progress Notes.
tetratetra says
synchronized cardioversion, at what amount of Jules, where is the link?
Jeff with admin. says
Here are the cardioversion voltage doses:
Pg. 118: “Initial recommended doses:
-narrow regular: 50-100 J
-Narrow irregular: 120-200 J biphasic or 200 J monophasic
-Wide regular: 100 J
-Wide irregular: defibrillation dose (not synchronized)”
All of this information is covered on the tachycardia algorithm page.
I hope this helps.
Kind regards, Jeff
elainepractitioner@gmail.com says
Is there a logical method for memorizing this detailed information, or is only necessary to understand?
Jeff with admin. says
It is mostly necessary to understand the concepts and be familiar with everything.
The repetition that is built into the website is also designed to help you become very familiar with all of the concepts.
Make sure that you go through all of the practice tests and maybe could scenarios i make sure that you go through all of the practice tests and maybe could scenarios. This will help reinforce everything that you learned in the knowledge base.
Kind regards,
Jeff
Nissar says
Hi Jeff
First of all thank you for your amazing work.
Do you have any tips on how to distinguish supraventricular tachycardia with aberrancy or LBBB from monomorphic ventricular tachycardia??
And should we give adenosine for monomorphic v tach in case it might actually be a supraventricular tachycardia with LBBB?
Thank Jeff
Jeff with admin. says
Even with a 12-Lead ECG it can be difficult to distinguish SVT with aberrancy from monomorphic VT. Here is a good article that will help: SVT with aberrancy vs. VT.
Adenosine can safely be given for regular, wide complex, monomorphic VT. Here is a good reference for the use of adenosine for wide complex tachycardia.
Kind regards,
Jeff
rrt student says
” Expert consultation is always advised, and if unstable, the ACLS tachycardia algorithm should be followed.”
Should this read stable instead of unstable?
stable- tachycardia algorithm
unstable- cardiac arrest algorithm
Jeff with admin. says
If the patient is unstable, there will not be time to obtain a consultation from an expert. The tachycardia algorithm should be implemented for unstable tachycardia and if the patient becomes pulseless then you would use the cardiac arrest algorithm. The tachycardia algorithm has two branches stable and unstable.
Kind regards,
Jeff
James says
Your website is great and very helpful! I am learning rapidly! I wanted to see if you could briefly provide some depth about Torsades. I know we give IV Mag over 1-2 minutes but do we defibrillate? I suppose if the patient was having intermittent torsades and was stable we would give the mag over 5-60 minutes. But if the patient is symptomatic, unresponsive, and pulseless? Would we defibrillate first then administer the mag after a shock?
Jeff with admin. says
You would defibrillate and then treat with magnesium after the shock. Continue the code per ACLS protocol while administering the Magnesium.
Kind regards,
Jeff
imoh5 says
Hello Jeff!
Wanted to ask about an unstable patient requiring synchronized cardioversion in a real scenario. We corrected his BP using inotropes and then cardioverted. I thought this may have been an unnecessary delay.
Do you have any comments on this? Is our priority to stabilise and correct for the 4H’s and T’s prior to cardioverting in this scenario to optimise the chance of a good outcome or is it to to follow protocol and shock? He was not significantly hypovolaemic to begin with, but has a normal systolic of 90 and a poor ejection fraction and ischaemic heart disease.
Also can you comment on optimizing ROSC in a different situation like arrest. I.e. any leeways for putting in potassium replacement via IV in setting of known hypokalaemia, delaying CPR to do same etc
imoh5 says
p.s. when we administered inotropes our indication was a systolic of 50, with evidence of compromise.
Jeff with admin. says
Cardioversion in the unstable patient should be the main priority. The primary reason for the low BP is the inefficient cardiac output related to the VT (I’m assuming this was VT). After cardioversion address H’s and T’s to ensure that there is less reoccurrence of the arrhythmia.
When dealing with an already diseased heart and multiple comorbidities your job of stabilization and post shock treatment will be important.
After ROSC, you would always search for ways to optimize the patient condition and avoid arrest reoccurrence. A thorough search for any underlying cause for the arrhythmia will be important. You would not delay emergent treatment for an unstable patient. Think about and treat H’s and T’s throughout the emergency process, but CPR and defibrillation are the two most important interventions when treating cardiac arrest. I hope this helps and answers your questions.
Kind regards,
Jeff