There are several other tachycardia rhythms that can be seen with both stable and unstable tachycardia. These rhythms include monomorphic ventricular tachycardia and polymorphic ventricular tachycardia both of which are wide-complex tachycardias.
Wide complex tachycardias are defined as a QRS of ≥ 0.12 second. Expert consultation should be considered with these rhythms.
These wide-complex tachycardias are the most common forms of tachycardia that will deteriorate to ventricular fibrillation.
Monomorphic Ventricular Tachycardia
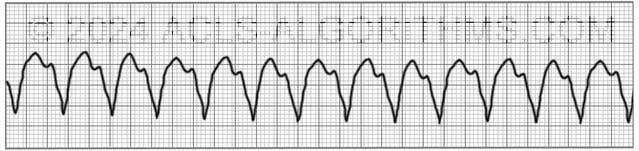
With monomorphic VT all of the QRS waves will be symmetrical. Each ventricular impulse is being generated from the same place in the ventricles thus all of the QRS waves look the same.
Treatment of monomorphic VT is dependent upon whether the patient is stable or unstable. Expert consultation is always advised, and if unstable, the ACLS tachycardia algorithm should be followed.
Polymorphic Ventricular Tachycardia
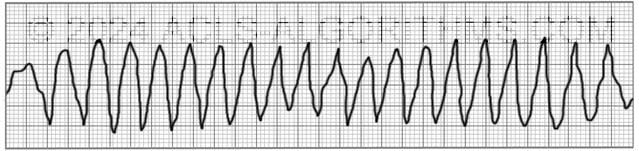
With polymorphic ventricular tachycardia, the QRS waves will not be symmetrical. This is because each ventricular impulse can be generated from a different location. On the rhythm strip, the QRS might be somewhat taller or wider.
One commonly seen type of polymorphic ventricular tachycardia is torsades de pointes. Torsades and other polymorphic VT are advanced rhythms which require additional expertise and expert consultation is advised.
If polymorphic VT is stable the ACLS tachycardia algorithm should be used to treat the patient. Unstable polymorphic ventricular tachycardia is treated with unsynchronized shocks (defibrillation). Defibrillation is used because synchronization is not possible.
These wide complex tachycardias tend to originate in the ventricles rather than like a normal rhythm which originates in the atria.
Top Questions Asked On This Page
-
Q: What are the doses for synchronized cardioversion?
A: Here are the cardioversion voltage doses:- Narrow regular: 50-100 J
- Narrow irregular: 120-200 J biphasic or 200 J monophasic
- Wide regular: 100 J
- Wide irregular: defibrillation dose (not synchronized)”
All of this information is covered on the tachycardia algorithm page.
-
Q: Is it necessary to memorize the doses listed above?
A: It is necessary to understand the concepts and be familiar with the shock dosages.
The repetition that is built into the website is designed to help you become very familiar with all of the concepts and use them in emergencies. -
Q: What sort of a pulse would you be feeling with a polymorphic VT?
A: You may feel a weak pulse or a strong pulse depending on how long the polymorphic VT has been going on. One thing is for sure….You won’t be feeling a pulse for very long if this rhythm continues.
veena says
AGAIN THANK YOU SO MUCH!!
veena says
wow evergrowing website.i would like to become a member.I am an RN and craving to work for cardiology unit and like to get a. handy(really small) ecg book in the pocket for reference
Ann Barber says
This site has been more helpful to me than anything I have ever studied! Thank you!
Grape123 says
Agreed!
LYNDA BLAKE says
Totally Agree. Lynda
ranwan51 says
I love this site! I have been ACLS certified for many years but I have to start studying at least one month prior. I work in an outpatient setting and do not have the opportunity to even see rhythms anymore. I hate reading the book every 2 years. I am going to use everything on your site. In what order do you suggest I begin this endeavor? Thanks, Old but not dead yet.
Jeff with admin. says
Here is a link to the “study guide” for the site. Hope it helps. Kind regards, Jeff
Dara Bass says
For Monomorphic VT would that pt be stable? what do you do for stable pt. Loving the site thanks so much!!!!
Jeff with admin. says
Monomorphic VT can be stable or unstable. It would depend on the patients signs and symptoms.
Treatment for both stable and unstable tachycardia can be found on this page:
Click where it says “Tachycardia Algorithm Diagram” and you can look at a flowchart that shows interventions.
Kind regards,
Jeff
Tom McGuinness says
Fantastic site for people who can speak english and can also read and understand english. Well worth every penny is costs. Thank you guys from all who have gained so much from this entire experience!
bethdubois says
Hi Jeff,
What is the difference between cardioversion, defibrillation, and synchronization?
Thanks,
Beth
Jeff with admin. says
This web page, “synchronized vs. unsynchronized cardioversion“, covers your question.
deecanales says
As a physician working on a rapid response team I could say this is the best acls review website ever. Keep up the good work guys!!
Joyce Rineer says
I know that I will be well prepared for my ACLS exam great learning environment
Dr, Gihan says
This site is so helpful and comprehensive, really great site.
Cecelia says
WOW! I am sooo elated that I now understand this type of Tachycardia…I”m loving this site….
ghulam mahdi says
Really very helpful ,i got fruitful result. i would like to my colleagues to get help from this site.
Mary says
I found this site extremely helpful, making it easier to understand the physiology behind the rhythms. Thanks so much!!!
Essam says
No way it is an esteemed website , but i wonder why for sudden of all it became paid site so it starts to loose its humanitarian GOAL . Still i remember 2 years back no site could compete it .Where it was free of charge.
I hope to go back to its non commercial message .
Nneka Mbadiwe says
say what?
tracy says
please don’t leave nasty comments about this extremely professional, well done, accurate, and helpful website until you can learn proper English and grammar. You should be ashamed to show people how inadequate your education is, and I’m frightened to think that you’re actually taking care of patients with so little intelligence.
Mary says
Essam, this site is not an entitlement.
Jacob Gaik says
All I know is, as a professional, I would have paid 10 x what I did for this site! I was confident before but I am still learning a lot here. Great site, great info, great format, and I am having a great experience! Thank guys!
Connie Schwendeman says
It never ceases to amaze me that the people who seem to criticize the most are the least intelligent. This is a very helpful website. Ignore the ignorant.
frog11 says
Essam: I think this site has a LOT of info for free and I am happy to pay for the additional Mega code videos especially since that is the most stressful part of taking ACLS. I think Jeff and Chris deserve some compensation for all they do to make this a comprehensive useful site. After perusing this site for 2days, I must say that I have a better understanding of it all than I previously had in 40+ years of nursing. I am grateful I stumbled upon this great website.
J. Harter says
As for diagnosing using Adenosine vs. Cardizem (this is what our agency carries for anti-arrythmics, along with Lido) on wide/borderline-wide complex tachycardias. We typically run a twelve lead ASAP w/initial supportive care obviously due to the cardiac complaint. Using the twelve lead we assess the PRI reading that is printed at the top since this reads out to the thousandths and we can only read the “little” boxes out to the hundreth. We look for a number and then have a bit more educated decision as to supraventricular vs ventricular origination. Any numerical data at PRI would more than likely indicate supra and you could more decisively adjust your treatment. Assess, supportive care, 12 lead and IV in conjunction with one another. We do this regularly and like a code our team falls into place to get things done. All things being equal for a stable and <48 hrs Pt complaint. Great site, love the material.
*Any thoughts?