Atrial flutter is an abnormal heart rhythm that technically falls under the category of supra-ventricular tachycardias. Atrial flutter is typically not a stable rhythm and will frequently degenerate into atrial fibrillation.
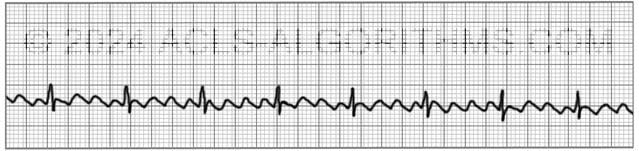
Atrial Flutter will usually present with atrial rates between 240-350 beats per minute. These rapid atrial rates are caused by electrical activity that moves in a self-perpetuating loop within the atria.
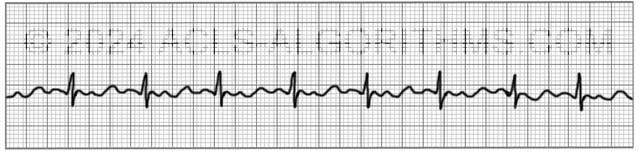
The impact and symptoms of atrial flutter depend upon the ventricular rate of the patient (i.e. cardiac output). Usually, with atrial flutter, not all of the atrial impulses will be conducted to the ventricles, and the more atrial impulses that are conducted, the greater the negative effect.
Symptoms
Symptoms of atrial flutter are similar to those of atrial fibrillation and may include the following:
- palpitations, chest pain or discomfort
- shortness of air
- lightheadedness or dizziness
- nausea
- nervousness and feelings of impending doom
- symptoms of heart failure such as activity intolerance and swelling of the legs occur with prolonged fast flutter)
Complications
As with its symptoms, atrial flutter shares the same complications as atrial fibrillation. These complications are usually due to ineffective atrial contractions and rapid ventricular rates. Ineffective atrial contractions can lead to thrombus formation in the atria and rapid ventricular rates can cause decompensation and heart failure.
Prevent complications from atrial flutter with early cardioversion.
Treatment
For the purposes of ACLS, atrial flutter is treated the same as atrial fibrillation. When atrial flutter produces hemodynamic instability and serious signs and symptoms, it is treated using ACLS protocol.
For the patient with unstable tachycardia due to this tachyarrhythmia (atrial flutter), immediate cardioversion is recommended. Drugs are not used to manage unstable tachycardia.
Cardioversion
Atrial flutter is considerably more sensitive to electrical direct-current cardioversion than atrial fibrillation, and usually requires a lower energy shock. 20-50J is commonly enough to revert to sinus rhythm.
AHA recommends an initial shock dose 0f 50-100 J for cardioverting unstable atrial flutter.
Below is a short video which will help you quickly identify atrial flutter on a monitor.
Please allow several seconds for the video to load. (3.84 mb)
Click for next Rhythm Review: Atrial Fibrillation
Questions Asked On This Page
-
Q: What are the chances of the formation of thrombus in the atrial cavity in the case of long-standing atrial flutter? Do we have to give anticoagulation, as in atrial fibrillation, to minimize the risk of emboli?
A: The chances for thrombus formation are relatively high. You would want to perform a TEE to ensure that there is no thrombus formation and you would want to initiate anticoagulation therapy.
-
Q: Energy levels for cardioversion of unstable a-flutter with both biphasic and monophasic devices? I haven’t seen anything as low as 20-50 joules mentioned in the AHA material, but I’m just getting started.
A: Unstable atrial flutter is treated as an unstable tachycardia within the tachycardia algorithm. Synchronized cardioversion is indicated, and the starting dose for narrow, regular tachycardia would be 50 J.
The page which states that 20-50 J can is used for the conversion of atrial flutter is speaking about atrial flutter in general and this could mean both stable and unstable atrial flutter.
Studies have shown that lower doses between 20-50 J are adequate for the conversion of atrial flutter. -
Q: I would assume that atrial flutter always has a rate more than 240. Are there any other rhythms that have rates that high? If not that might be one way to help identify flutter when not a sawtooth pattern.
A: Atrial flutter does not always have such a high atrial rate, but it usually will. Remember that flutter will many times only affect the atrial rate.
The ventricular rate may still be relatively low but usually more than 100. Symptoms will be seen when the ventricular rate is affected or if the patient develops a blood clot due to the pooling of blood in the atria related to the ineffective fluttering.
VT can have rates more than 240 but in this situation, the patient will most likely be pulseless, and you will treat using the cardiac arrest algorithm.
Usually, you will recognize atrial flutter by consistent saw-tooth or wave-like pattern between the QRS complexes.
Judith C Marlar says
As a medic, if I determine the condition to possibly be 48 hours old, should I administer aspirin before Cardioversion ?
Jeff with admin. says
You would not want to perform cardioversion in the field with the patient that has been in atrial flutter or atrial fibrillation for any length of time. The patient is most likely stable. The patient should be evaluated by a cardiologist prior to any intervention.
If the patient has not been anticoagulated, there’s a good chance that she could have a thrombus. A (TEE) transesophageal echocardiogram should be performed prior to cardioversion in this type of situation.
If cardioversion is performed in this type of situation, it should be in a controlled hospital setting.
If they are not stable, there are serious risks to performing cardioversion if the onset of the atrial fibrillation or atrial flutter is unknown. If possible perform TEE. Aspirin will be of no value.
Kind regards,
Jeff
Liliana Gutierrez says
Just curious why you call it Shortness of Air instead of Shortness of Breath (SOB) as we document it in clinical settings.
Jeff with admin. says
Either one is fine. In the region where I work, “short of air” or “shortness of air” has become the commonly used wording for someone that is having difficulty breathing. There are some areas of the country that still use “short of breath” or “shortness of breath.” Either is fine and both are widely accepted to describe someone who is having difficulty breathing.
Kind regards, Jeff
Benham Pruett says
I have some issues with your response to question 11. One, the Vagus nerve also innervates the SA node, not only the AV node as stated…vagal maneuvers do more than just affect the AV node. Two, afib and aflutter are technically a Supra Ventricular Tachycardia (SVT) and can absolutely be treated with vagal maneuvers. However, my understanding is that vagal maneuvers for aflutter have no efficacy as of late.
You stated that “Atrial fib and atrial flutter originate in the atria so vagal maneuvers, which have their affect on the AV node, would only slow the rate of conduction of the afib or aflutter.” That is literally what happens with every SVT when you do vagal maneuvers, you just get lucky as to whether or not it works to convert the patient and keep them converted. You can even convert a stable SVT or afib RVR with a fluid bolus.
Tell me if I’m wrong, but that is my understanding.
Thanks.
Jeff with admin. says
One, the Vagus nerve also innervates the SA node- not only the AV node as stated…vagal maneuvers do more than just affect the AV node.
(Jeff’s response-I agree. My exclusion of the other things that the vagus nereve innervates was to simplify the explaination.)
Two, afib and aflutter are technically a Supra Ventricular Tachycardia (SVT) and can absolutely be treated with vagal maneuvers.
(Jeff’s response- if there is no efficacy for treatment of AF with vagal maneuvers, it shouldn’t be used.)
You stated that “Atrial fib and atrial flutter originate in the atria so vagal maneuvers, which have their affect on the AV node, would only slow the rate of conduction of the afib or aflutter.” That is literally what happens with every SVT when you do vagal maneuvers, you just get lucky as to whether or not it works to convert the patient and keep them converted. You can even convert a stable SVT or afib RVR with a fluid bolus.
(Jeff’s response- It’s not luck. The term SVT is overused. The most common form of SVT that is narrow, regular, and >150 is AVNRT, where the accessory pathway lies in the AV Node. In this case vagal maneuvers will allow time for the AV node to depolarize, eliminating the accessory pathway’s use as a pathway, then allowing the sinus node to resume pacemaker
Kind regards, Jeff
Joseph says
Wow????sweetly precise. Written in a way to favor us the *slow* learners????
Janet Go says
Hi Jeff,
I took care of this very sick patient before, his rhythm was in A-fib RVR and converted to A-Flutter with 140-145 bpm and stayed there almost my whole shift, the patient’s BP was okay nothing too low although I can tell patient is not feeling very well at some point he was feeling dizzy or having discomfort. The patient has cardizem and amiodarone drip on top of his protonix, TPN etc.. it was crazy how many things is going on with the pt. I was frequently on the phone with the hospitalist and cardiologist. I finally asked the cardiologist whether other treatments can possibly be done for the pt. like cardioversion?(I hinted), the cardiologist replied he does not want to do the procedure because pt. may end up having stroke. I looked it up but just wanting to know your thoughts about this matter. BTW, the patient was in A-Fib CVR the next day with no cardioversion done. Thanks
Janet Go says
Well, what do you know I found the reason to why the cardiologist said NO to cardioversion. I was reading the A-Fib part of the lesson and it says in there: “Cardioversion of stable atrial fibrillation should be performed with caution if the arrhythmia is more than 48 hours old and no anticoagulant therapy has been initiated due to the risk of emboli that can cause MI and stroke”. This make sense to my pt. condition since we stopped anti coagulants due to high rick of bleeding because of another medical condition the pt. have (severe inflammation OR possible ischemic gut that’s needing immediate surgical procedure). I like how the lessons are set up here. Thanks for sharing your knowledge.
Jeff with admin. says
There is a risk that a patient in atrial
fibrillation or atrial flutter could have a thrombosis break loose and cause a stroke when cardioversion is performed. Thrombus can form in the heart due to the fibrillating /fluttering nature of the atria if the patient has not been anticoagulated.
Typically a transesophageal echocardiogram is performed prior to any cardioversion. This is used to rule out thrombus. Once thrombus ruled out, cardioversion can be performed.
Kind regards,
Jeff
amy says
If somebody had A Flutter with a rate of 70 bpm and no symptoms, would they be required to go into hospital with a time-critical transfer or just go in normally?
Similarly, if the patients heart rate was over 100, for example 150bpm and was not symptomatic, would they require a time-critical transfer or just a normal transfer to hospital?
Thanks
Amy
Jeff with admin. says
Non-symptomatic atrial flutter would not be considered a cardiac emergency and would not require time critical transfer. If the patient had symptoms such as dizziness, lightheadedness, chest pain, or low blood pressure then this would become a cardiac emergency and we need time critical transfer.
In the case that there are no symptoms, treatment as soon as possible would be needed however, it would not be considered an emergency or time critical. Urgent would be a more appropriate term.
Kind regards,
Jeff
Amy says
With a non-symptomatic patient with A Flutter should a time-critical transfer be taken to hospital?
Jeff with admin. says
For non-symptomatic atrial flutter, this would not require a time critical transfer. It would be important to take care this as soon as possible, but it would not be considered a cardiac emergency.
Kind regards,
Jeff
TALAL HAWSAWI says
Hi Jeff
What should be done with the patient having a symptomatic AF with thrombus found in the atria ?
What the management for stable A.flutter and A. fibrillation?
Jeff with admin. says
If the patient is symptomatic because the heart rate is too fast then you would slow the heart rate with something like a calcium channel blocker or beta blocker. You would also anticoagulate the patient.
If the patient is symptomatic because the heart rate is too slow then you would treat with the bradycardia algorithm.
Kind regards,
Jeff
Steve Hinze says
Jeff! I think what you are doing is a ministry!! Thankyou!! Steve
Jeff with admin. says
Thank you, Steve. It definitely is, and it is my privilege to serve this healthcare community. Kind regards, Jeff
lullrich says
Hi Jeff –
In the explanation above about how to stabilize a patient in aflutter, it says … Aflutter usually requires a lower energy shock of 20-50J. This shock dose is commonly enough to revert aflutter to sinus rhythm. In the box below that it says: AHA: Recommends an initial shock dose of 50-100J for cardioverting unstable aflutter. So, I’m thinking that if, during a code, aflutter had to be cardioverted, the lower shock can be used, but for purposes of the ACLS course, the answer would be a shock dose of 50-100J. Why would we use a higher energy shock dose if a lower shock dose would be sufficient? Thanks again. Linda
Jeff with admin. says
AHA makes the recommendation of 50-100 J specifically for unstable atrial flutter.
In the web page, I was just stating the fact that atrial flutter is much more sensitive to electricity and 20-50 J is usually sufficient for conversion.
For the purposes of unstable atrial flutter start at 50 J and go up from there.
Kind regards,
Jeff
MAHESH KUMAR says
i have a question that a patient admitted with atrial flutter with normal ventricular rate 92 beat per minute and after the post of mitral valve replacement still had atrial flutter
so whether that kind of patient can be shifted out of the ICU ?
Jeff with admin. says
It would depend upon your hospital protocol and how conservative the cardiac surgeon performing the surgery is. A step down unit or telemetry unit would most likely be sufficient for this patient postoperatively.
Kind regards,
Jeff
marisa says
Isn’t flutter a Right heart disease? wouldn’t MV repair just fix a fib and not flutter?
thanks
marisa
Leah says
I am doing a study on The new modified Valsalva maneuver to treat supraventricular tachycardia and I notice that all the studies I can find exclude patients with Atrial Fib, Atrial Flutter and Sinus Tachycardia, yet no one explains why. Are Vagal maneuvers at all effective in converting Atrial Fib, Atrial Flutter? If not, why…and if they are, why do you think these conditions are excluded from so many of the studies on Valsalva. Thank you for your time.
Jeff with admin. says
No, vagal maneuvers are not effective to convert afib or aflutter. Atrial fib and atrial flutter originate in the atria so vagal maneuvers, which have their affect on the AV node, would only slow the rate of conduction of the afib or aflutter. Maneuvers would not fix the afib or flutter arrhythmia problem.
SVT is effectively treated with vagal maneuvers approx. 25% of the time because the increased vagal tone and slowing conduction can cause AVNRT/AVRT conversion and reestabilish the normal AV node pathway of electrical conduction.
Does that make sense?
Kind regards,
Jeff
Xaara Xaara says
For a patient with stable A-flutter, can they be put on dose of calcium channel blockers or ARBs?
How often should they be evaluated as out patient when on tx?
I fail to understand the effectiveness of the role of adenosine.
Thanks
Jeff with admin. says
Adeonsine is typically used for the treatment of stable SVT and stable SVT with symptoms.
You may use adeonsine as a diagnostic tool to slow down the heart to identify atrial flutter or fibrillation, but adenosine will not “fix” atrial fibrillation or atrial flutter.
Calcium channel blockers in the setting of ACLS are used to slow down the ventricular heart rate. This can help eliminate an unstable condition but it will also not “fix” the flutter or fibrillation.
There are many underlying causes for atrial flutter and atrial fibrillation. You would want to ensure that you have attempted to treat the cause of the problem to fix the problem. If the cause cannot be determined anticoagulants can be used to decrease the risk of clot formation. Also, if the problem cannot be corrected or controlled, ablation can be performed to relieve symptoms and improve quality of life.
Kind regards,
Jeff
prafulz says
Hi Jeff,
How to treat stable atrial flutter? What medication one should give in patient of stable atrial flutter?
Jeff with admin. says
Radiofrequency catheter ablation is now the long-term treatment of choice in patients with symptomatic atrial flutter.
Kind regards,
Jeff
2livewell says
Hi Jeff
Love your site. I am back studying for my recert.
I understand Aflutter is treated with cardioversion 50-100J.
Question: a patient maintain “A-Flutter” controlled (similar to Afib controlled –100 bpm or less)?
Is there a sustained controlled rate of A-flutter? I do understand that Aflutter can lead to thrombus formation…reason being recently I was relieving our monitor tech and a patient was in A-Flutter apparently all night and the rate ranged from 80-110 and apparently patient was at this rate and rhythm for 24 hours.
Thank you for your feedback!
2livewell says
Meant to say “Can a patient maintain A Flutter”
Jeff with admin. says
Yes a person can maintain a normal ventricular rate and remain in atrial flutter for quite a long time. Some people live with this condition just as with atrial fibrillation. You might see a person with a controlled atrial flutter that is 1:2 or 1:3. This means that for every one ventricular impulse, there is either two or three atrial impulses. To remain stable, the ventricular rate would need to be consistently less than 100. Rates higher than this would be dealt with through the use of medications or some type of cardiovascular intervention. Kind regards, Jeff