Atrial flutter is an abnormal heart rhythm that technically falls under the category of supra-ventricular tachycardias. Atrial flutter is typically not a stable rhythm and will frequently degenerate into atrial fibrillation.
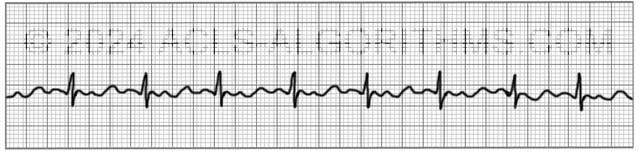
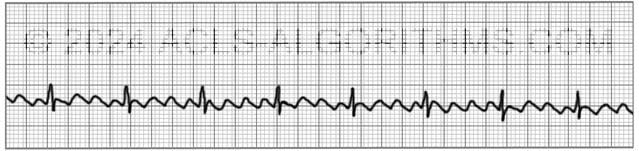
Atrial Flutter will usually present with atrial rates between 240-350 beats per minute. These rapid atrial rates are caused by electrical activity that moves in a self-perpetuating loop within the atria.
The impact and symptoms of atrial flutter depend upon the ventricular rate of the patient (i.e. cardiac output). Usually, with atrial flutter, not all of the atrial impulses will be conducted to the ventricles, and the more atrial impulses that are conducted, the greater the negative effect.
Symptoms
Symptoms of atrial flutter are similar to those of atrial fibrillation and may include the following:
- palpitations, chest pain or discomfort
- shortness of air
- lightheadedness or dizziness
- nausea
- nervousness and feelings of impending doom
- symptoms of heart failure such as activity intolerance and swelling of the legs occur with prolonged fast flutter)
Complications
As with its symptoms, atrial flutter shares the same complications as atrial fibrillation. These complications are usually due to ineffective atrial contractions and rapid ventricular rates. Ineffective atrial contractions can lead to thrombus formation in the atria and rapid ventricular rates can cause decompensation and heart failure.
Prevent complications from atrial flutter with early cardioversion.
Treatment
For the purposes of ACLS, atrial flutter is treated the same as atrial fibrillation. When atrial flutter produces hemodynamic instability and serious signs and symptoms, it is treated using ACLS protocol.
For the patient with unstable tachycardia due to this tachyarrhythmia (atrial flutter), immediate cardioversion is recommended. Drugs are not used to manage unstable tachycardia.
Cardioversion
Atrial flutter is considerably more sensitive to electrical direct-current cardioversion than atrial fibrillation, and usually requires a lower energy shock. 20-50J is commonly enough to revert to sinus rhythm.
AHA recommends an initial shock dose 0f 50-100 J for cardioverting unstable atrial flutter.
Below is a short video which will help you quickly identify atrial flutter on a monitor.
Please allow several seconds for the video to load. (3.84 mb)
Click for next Rhythm Review: Atrial Fibrillation
Questions Asked On This Page
-
Q: What are the chances of the formation of thrombus in the atrial cavity in the case of long-standing atrial flutter? Do we have to give anticoagulation, as in atrial fibrillation, to minimize the risk of emboli?
A: The chances for thrombus formation are relatively high. You would want to perform a TEE to ensure that there is no thrombus formation and you would want to initiate anticoagulation therapy.
-
Q: Energy levels for cardioversion of unstable a-flutter with both biphasic and monophasic devices? I haven’t seen anything as low as 20-50 joules mentioned in the AHA material, but I’m just getting started.
A: Unstable atrial flutter is treated as an unstable tachycardia within the tachycardia algorithm. Synchronized cardioversion is indicated, and the starting dose for narrow, regular tachycardia would be 50 J.
The page which states that 20-50 J can is used for the conversion of atrial flutter is speaking about atrial flutter in general and this could mean both stable and unstable atrial flutter.
Studies have shown that lower doses between 20-50 J are adequate for the conversion of atrial flutter. -
Q: I would assume that atrial flutter always has a rate more than 240. Are there any other rhythms that have rates that high? If not that might be one way to help identify flutter when not a sawtooth pattern.
A: Atrial flutter does not always have such a high atrial rate, but it usually will. Remember that flutter will many times only affect the atrial rate.
The ventricular rate may still be relatively low but usually more than 100. Symptoms will be seen when the ventricular rate is affected or if the patient develops a blood clot due to the pooling of blood in the atria related to the ineffective fluttering.
VT can have rates more than 240 but in this situation, the patient will most likely be pulseless, and you will treat using the cardiac arrest algorithm.
Usually, you will recognize atrial flutter by consistent saw-tooth or wave-like pattern between the QRS complexes.
Andrew Starr says
If a patient is unstable, by definition, the patient is at risk of death by low perfusion and low cardiac output. Would a practitioner then use synchronized cardioversion without checking for a thrombus? Doing a TEE sounds like a luxury for a stable patient. Thanks for your help!!
ACLS says
If a patient is unstable due to atrial fibrillation or other tachyarrhythmias, synchronized cardioversion would be performed without first checking for a thrombus using transesophageal echocardiography (TEE).
The rationale for this approach is as follows:
Kind regards,
Jeff
Tippi says
Usually, with atrial flutter, not all of the atrial impulses will be conducted to the ventricles. The more atrial impulses that are conducted, the greater the negative effect.
Can you please explain further why conducted atrial impulses have a negative effect?
And “NOT ALL” of the atrial impulses will be conducted to the ventricles? Where do these other impulses go?
ACLS says
The reason why conducted atrial impulses, have a negative effect is because this increases the ventricular rate. The ventricular rate can become so rapid that ventricular filling is inhibited. This leads to less oxygen, and nutrients being supplied to the organs and tissues of the body.
Some of the impulses are blocked at the AV node, a bundle of cells in the upper wall of muscle between the ventricles, your heart’s lower chambers. It usually slows the beats by a fourth or a half, or down to somewhere between 150 and 75 beats per minute.
Kind regards,
Jeff
Dzina Rozava says
I have a question. In the event of a stable, but persistent A-fib/A-flutter, we have time to do TEE to rule out clots and start an anticoagulation therapy, before cardioversion or even potential ablation. However if patient decompensates before TEE is obtained, we can’t use cardioversion, will amiodarone or other medication be appropriate at this point? What are the options in that case? Or our focus of treatment changes towards declotting protocols? Thank you.
ACLS says
Amiodarone or other medication’s like Calcium channel blocker’s and beta blockers could be potential appropriate medication’s in the situation is.
Fortunately, atrial fibrillation and atrial flutter rarely in and of themselves lead to decompensation that could result in cardiac arrest.
Kind regards,
Jeff
Derek Longoria says
As a paramedic… if I came across stable atrial flutter in the field would there be any interventions that I would do? The closest thing I think I can get to is considering calcium channel blockers but if the pt is stable… should I just wait until I get the pt to the hospital?
ACLS says
In the situation where you were dealing with stable atrial flutter, the best thing to do would be to wait until you get to the hospital so that a more thorough evaluation and consultation may be performed.
The main thing you’re looking at here would be the stable condition. When a patient is stable, you have time to allow more experienced providers to perform an evaluation prior to interventions.
Kind regards,
Jeff