
Second degree heart block which is also called Mobitz 1 or Wenckebach is a disease of the electrical conduction system of the heart in which the has progressive prolongation until finally the atrial impulse is completely blocked and does not produce a QRS electrical impulse.
Once the p-wave is blocked and no QRS is generated, the cycle begins again with the prolongation of the PR interval.
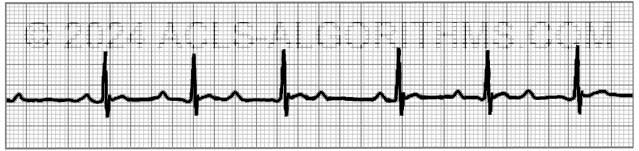
One of the main identifying characteristics of second-degree AV block (Type 1) is that the atrial rhythm will be regular.

In the above image, notice that the p-waves are regular, the PR-interval progressively gets longer until a QRS is dropped and only the p-wave is present.
PR Interval
The PR interval is the electrical firing of the atria and conduction of that electrical impulse through the AV node to the ventricles.
Although second-degree AV block (Type 1) is not typically clinically significant for ACLS, recognition of the major AV blocks is important because treatment decisions are based on the type of block present.
Second-degree AV block (Type I) may be a normal variant in the conduction system of the heart and is usually due to a reversible conduction block at the level of the AV node. There are several disorders that can cause Second-degree AV block (Type I). The most common causes are listed below:
Causes of Second-degree AV block (Type I):
- Increased vagal tone (well trained athlete)
- Medications that inhibit AV node conduction (amiodarone, beta-blockers, calcium channel blockers, digoxin)
- Myocarditis caused by infections
- Hypoxemia (see more in infants and children)
- Cardiac surgery
- Myocardial infarction
- Any condition that stimulates vagal tone
Below is a short video which will help you quickly identify second-degree AV block (Type 1) on a monitor. Please allow several seconds for the video to load. (3.69 mb)
Click for Next Rhythm Review:
Second Degree AV Block (Type II)
Top Questions Asked On This Page
-
Q: In second degree AV block what is the meaning of “QRS dropped?” Does it mean less than 3 square?
A: It means that the QRS is not present. You will most likely see a p-wave but no QRS. The impulse that is produced in the SA node (p-wave) is not transferred through the AV node, and therefore no QRS wave is seen on the monitor.
-
Q: With 2nd-degree Type I, is atropine warranted or should we go straight to pacing?
A: Atropine should come before the application of pacing as long as the administration of atropine will not delay the use of pacing in an unstable patient.
-
Q: Why would the ventricle not fire a beat following the AV node non-conductive beat/ p wave non-conductive beat?
A: 2nd Degree Block Type 1 (Mobitz I) is usually due to a reversible conduction block at the level of the AV node. Some of the reversible causes are caused by medications such as beta-blockers, calcium channel blockers, and digoxin. Other reasons are inferior MI, myocarditis, increased vagal tone, and post heart surgery.
The AV node cells are malfunctioning, and they tend to fatigue progressively until they fail to conduct an impulse.
Teresa says
I had a patient in Mobitz 1 rhythm at a rate of 60. She was frightened “to death” about the test anyway and I told her if she refused the test that was her decision. The doctor didn’t really give her an informed consent because I think he thought it would scare her out of the Lexi more. I told her don’t do it. Her symptoms were very atypical and the doctor told her that he didn’t think it was her heart. She could then see her cardiologist and come back as an outpatient. Actually my question is what is the danger of Lexiscan in this rhythm?
Jeff with admin. says
The danger would be minimal. As with any test utilizing a medication, there are possible side effects that may be experienced.
“The most common side effects that occurred in clinical trials of Lexiscan were shortness of breath, headache, flushing, chest discomfort or chest pain, dizziness, nausea, abdominal discomfort, a metallic taste in the mouth, and feeling hot. Most common side effects began soon after receiving Lexiscan and went away within 15 minutes except for headache, which resolved in most patients within 30 minutes.” Quote found here.
Kind regards,
Jeff
ls1581 says
Why is TCP the treatment for Mobitz Type II because a dropped QRS = no circulation but on a Mobitz I, the PR lengthens and results in a dropped QRS but there is usually no treatment needed????
Jeff with admin. says
TCP is the treatment of choice for Mobitz Type II because this rhythm does not usually respond well to atropine. Also, Mobitz II will usually be associated with symptomatic bradycardia. Mobitz I will not usually be associated with symptoms or an unstable condition (it is usually benign).
Kind regards,
Jeff
Amber says
I think I need some clarification too.
The dropped QRS in Mobitz II = no circulation. Does the dropped QRS in Mobitz I also present the same danger?
Please help me understand. It seems to me that both are concerning.
By the way, your site has been very helpful for me. Thank you for your work on this website. I have already recommended it to several colleagues.
Jeff with admin. says
Unlike Mobitz I, which is produced by progressive fatigue of the AV nodal cells, Mobitz II is an “all or nothing” phenomenon whereby the His-Purkinje cells suddenly and unexpectedly fail to conduct a supraventricular impulse. Mobitz II is much more likely than Mobitz I to be associated with hemodynamic compromise, severe bradycardia and progression to 3rd degree heart block.
With Mobitz I, after the dropped beat, the process of progressive fatigue and dropped beat starts over. This makes Mobitz I a much safer bradyarrhythmia. With Mobitz II, the conduction can fail and it may no long conduct an impulse (Third degree block). This makes Mobitz II a very dangerous rhythm which must be dealt with as soon as possible.
Kind regards,
Jeff
aclsnursewh says
So helpful when I can replay the rhythms. I am learning quite a bit from watching the videos. Looking forward to more.
okeyi2000 says
I probably don’t see what others see in this diagram ! where is the dropped beat ,how do you distinguish that from the T wave? The prolongation is clear but can someone show me where we are missing a QRS.
Jeff with admin. says
The dropped beat is the first p-wave in the diagram and the p-wave that is almost in the middle of the image.
The 2nd non-conducted p-wave occurs on the t-wave after a QRS.
Kind regards,
Jeff
MCKINNEY says
GOOD TO BE ABLE TO REPLAY THIS OVER AND OVER UNTIL YOU GET IT
sonlis says
Love this site..it is very helpful!
Brenda Biancosino says
Don’t forget the helpful phrase we all learned in nursing school: “Longer, longer, longer, DROP, then we have a Wenckebach”.
Studying this weekend to recertify for the first time. Love your site. Thank you for all your hard work to make this an enlightening experience as well as reducing my stress level.
I have already recommended your site and will continue to do so.
Dan says
Thank you Brenda ! I personally love mnemonics. They free me up from that momentary ” pause” ( no pun intended) in the thought process that usually leads to a complete block ( again, no pun intended) in my review. If you have one for the Glascow Coma Scale that would be fantastic!
janetalucas says
Yes, Brenda that is helpful!
Albert EMT-P says
I teach Going, Going, Gone. It’s a phrase we all know and grew up with.
Albert EMT-P says
And, this is a great site. I just found it today and will make a note to show my EMT-P students at the college. I know this will help them in more ways than one.
poonam says
This makes total sense..It gave me a clear understanding of my strips..thanks so much
michell says
This so ROCKS!!!! I can actually make sense of these strips! Big ThanK YOU
Jack says
(1) The SA Node is the hearts primary pacemaker. (2) The SA Node generates an impulse which propagates across/thru the atria and to the A/V Node in attempt to cause the stimulation to the ventricles (via the Bundle of His and then the Purkinje Fibers. (3) The A/V Nodes primary function is to figuratively act as a gatekeeper as if there was a little man standing there with his hand on the gate allowing signals to pass thru in such a way that optimizes the hearts contracting as a smooth functioning unit (this ensures the greatest movement of blood thru the heart chambers and sets the stage for the greatest EF from the left ventiricle). (4) In the case of heart block the gatekeeper is (for some physiologic reason) restricting the passage of necessary stimulations from above the A/V Node (in the best case scenario the SA Node) from passing thru his gate so that they can transfer their stimulus to the ventricles. (5) If the QRS’s are narrow the block is in the A/V Node (internodal), if the are QRS’s wide (aberrant conduction) then the block is below the A/V Node and somewhere in the Bundle of His or Bundle branches which is much more serious and could ultimately lead to 3rd degree block and will typically create hemodynamic issues for the patient. The MD will most likely end up installing an artificial pacemaker in the patient to safegaurd the possibility of more serious heart failure.
miriam belo tan says
Agreat site. Clear & simple . Makes it fun to study.
Craig Jenkins says
why would the ventricle not fire a beat following the AV node non conductive beat/ p wave non conductive beat?
Jeff with admin. says
2nd Degree Block Type 1 (Mobitz I) is usually due to reversible conduction block at the level of the AV node. Some of these are medications such as beta-blockers, calcium channel blockers, and digoxin. Other causes are inferior MI, myocarditis, increased vagal tone, and post heart surgery.
Essentially the AV node cells are malfunctioning and tend to progressively fatigue until they fail to conduct an impulse.
Kind regards,
Jeff
tom barry says
Jeff 2nd degree type one, is atropine warranted or go straight to pacing?
Jeff with admin. says
The use of atropine should come before the use of pacing as long as the use of atropine will in no way delay the use of pacing in an unstable patient.
Kind regards,
Jeff
marshall williams says
thank u info very helpfull
Grape123 says
With second degree type one seems like there is a qrs after ea p wave it’s just prolonged where with second degree type two there is no qrs. after every p . having trouble with these blocks.
Jeff with admin. says
The two statements above are correct. You are getting it. Great job!
Kind regards,
Jeff
jonathanjung says
Hi Jeff, I don’t understand your answer to Grape123. Grape123 said “With second degree type one seems like there is a qrs after ea p wave it’s just prolonged “. You seemed to agree with that. I thought the P to P interval is constant and PR interval is increasing and then eventually a QRS is dropped. Is this not the case? Also, if I am correct about the QRS being eventually dropped, is this because the P is to close to the QRS and the ventricle has not had time to repolarize? Thanks
Jeff with admin. says
You are correct. I misread Grap123’s question. 2nd degree Type 1 the P to P interval is constant and the PR interval is progressively prolonged until the QRS is dropped and only the p-wave is seen.
When the QRS is dropped it is because the impulse is not conducted to the ventricles. Most of the time this directly related to a conduction problem between the atria and ventricles and is not directly related to the timing of ventricular repolarization.
Kind regards,
Jeff
Code-hanadi says
In second degree Av block what’s mean of qrs dropped is it mean less then 3 sequare
Jeff with admin. says
It means that the QRS is not present. You will most likely see a p-wave but no QRS. The impulse that is produced in the SA node (p-wave) is not transferred through the AV node and therefore no QRS wave is seen on the monitor.
Kind regards,
Jeff