
Second degree heart block which is also called Mobitz 1 or Wenckebach is a disease of the electrical conduction system of the heart in which the has progressive prolongation until finally the atrial impulse is completely blocked and does not produce a QRS electrical impulse.
Once the p-wave is blocked and no QRS is generated, the cycle begins again with the prolongation of the PR interval.
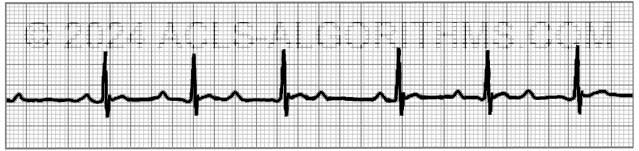
One of the main identifying characteristics of second-degree AV block (Type 1) is that the atrial rhythm will be regular.

In the above image, notice that the p-waves are regular, the PR-interval progressively gets longer until a QRS is dropped and only the p-wave is present.
PR Interval
The PR interval is the electrical firing of the atria and conduction of that electrical impulse through the AV node to the ventricles.
Although second-degree AV block (Type 1) is not typically clinically significant for ACLS, recognition of the major AV blocks is important because treatment decisions are based on the type of block present.
Second-degree AV block (Type I) may be a normal variant in the conduction system of the heart and is usually due to a reversible conduction block at the level of the AV node. There are several disorders that can cause Second-degree AV block (Type I). The most common causes are listed below:
Causes of Second-degree AV block (Type I):
- Increased vagal tone (well trained athlete)
- Medications that inhibit AV node conduction (amiodarone, beta-blockers, calcium channel blockers, digoxin)
- Myocarditis caused by infections
- Hypoxemia (see more in infants and children)
- Cardiac surgery
- Myocardial infarction
- Any condition that stimulates vagal tone
Below is a short video which will help you quickly identify second-degree AV block (Type 1) on a monitor. Please allow several seconds for the video to load. (3.69 mb)
Click for Next Rhythm Review:
Second Degree AV Block (Type II)
Top Questions Asked On This Page
-
Q: In second degree AV block what is the meaning of “QRS dropped?” Does it mean less than 3 square?
A: It means that the QRS is not present. You will most likely see a p-wave but no QRS. The impulse that is produced in the SA node (p-wave) is not transferred through the AV node, and therefore no QRS wave is seen on the monitor.
-
Q: With 2nd-degree Type I, is atropine warranted or should we go straight to pacing?
A: Atropine should come before the application of pacing as long as the administration of atropine will not delay the use of pacing in an unstable patient.
-
Q: Why would the ventricle not fire a beat following the AV node non-conductive beat/ p wave non-conductive beat?
A: 2nd Degree Block Type 1 (Mobitz I) is usually due to a reversible conduction block at the level of the AV node. Some of the reversible causes are caused by medications such as beta-blockers, calcium channel blockers, and digoxin. Other reasons are inferior MI, myocarditis, increased vagal tone, and post heart surgery.
The AV node cells are malfunctioning, and they tend to fatigue progressively until they fail to conduct an impulse.
amina says
in 2 degree type 1 does it means that block is at av node
Jeff with admin. says
That is correct.
Kind regards, Jeff
karenmargolin says
I can see from the monitor that the PR is longer, is it longer than type 1, and where on the strip does it show that the QRS is dropped.
Jeff with admin. says
The first dropped QRS is after the first P-wave in the strip. The second dropped QRS is after the 3rd visible QRS. Regards, Jeff
Yas-acls says
You said that in 2nd degree AV block, there is a dropped QRS. While watching the rhythm got the Type 2 Second Degree, the dropped QRS is more dropped in the literal meaning. What do you mean by dropped QRS on the 1st Second Degree Av block? Thank you.
Jeff with admin. says
“dropped QRS” means that atrial impulse (p-wave) is not conducted through the SA node and does not generate ventricular contraction (QRS wave).
Normally, with electrical conduction through the heart you will see a p-wave that represents atrial depolarization then you will see the QRS wave which represents ventricular depolarization. The action of atrial depolarization is supposed pass on through the SA node and potentiate the ventricular depolarization. The “dropped QRS” means that electrical conduction is blocked from traveling down through the SA node so there is no QRS. Kind regards, Jeff
nora says
Good day !
what I know is: The SA node is the dominant pacemaker cells in the heart ,These cells typically fire at a rate of 60 to 100 times per minute. But the electricity is conducted from atria to ventricls through the AV node by the Electrical conducting cells .
what u think?
Christina123 says
If the pt bp is low would they be considered unstable and symptomaic
Jeff with admin. says
If the blood pressure this would be considered symptomatic and it could go either way as far as being unstable or stable. The most common symptoms that indicate that the patient is unstable would be syncope, altered level of consciousness, chest pain, shortness or breath, weakness, light-headedness. If a patient has any of these symptoms with the low BP it would be considered unstable.—Jeff
Judy Taylor says
little confused here. If the p waves progressively lengthen how can they be regular?
Jeff with admin. says
The rate is regular. This would be the interval between QRS waves. —Regards, Jeff
Deanna says
Taking ACLS tomorrow. I wish I would have found this website sooner. Thanks a bunch!!!
Deborah says
Same here! How did it go?
Rochelle Galloway says
Why would you not pace a Mobitz 1 AV block?
Jeff with admin. says
If the patient is symptomatic with poor perfusion, you would pace. —regards, Jeff
Nursery says
I’ve never paced a patient with Winckebach. Wouldn’t the instability be due to something else??
Chris with admin says
It’s academic to differentiate between type 1 and type 2 second degree blocks in an emergency situation. The main concern would be the decrease in coronary perfusion due to the slow heart rate. The primary culprit for 2nd and 3rd degree blocks is acute MI. If the transcutaneous pacing is successful, it will immediately increase coronary perfusion and overall organ perfusion and gives you a stop gap to get the patient in for reperfusion therapy. Kind regards, Chris
joano says
Excellent visualization of this bradyarrhythmia. It can really be seen when placed against normal sinus rhythm.
larry r hill says
thanks again
Jodie Webb says
I love this website. Great info and easily understood. I do not think sound (beeping of HR) is needed…the pictures and videos with explanations are the important components. Great job on the whole format and website.
ANna Wistrom says
longer longer longer drop, now you have a Wenckebach
Lori says
Thanks for the little rhyhm…it helps 🙂
medina white says
They’re fine Jeff! Thank you! The pictures are worth a thousand beeps 😉
Holiday Jesse says
It might be useful to add the “beep beep beep” of the heart monitor. Kind of add to the realism.
Diane Johnson says
why isn’t there sound with these?
Jeff with admin. says
They were each so short, I opted for no sound. If you think that I should add something in the background, let me know. Jeff
Carrie Collier says
It helps to understand the different rhythms when they are compared at the same time. Thanks for taking the time to go over every aspect!