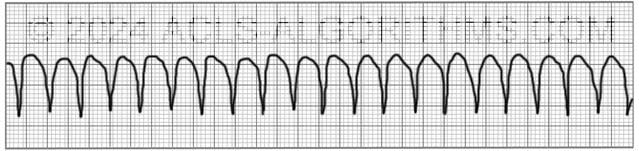
The pulseless ventricular tachycardia rhythm is primarily identified by several criteria. First, the rate is usually greater than 180 beats per minute, and the rhythm generally has a very wide QRS complex.
Second, the patient will be pulseless. And third, the rhythm originates in the ventricles. This is in contrast to other types of tachycardias which have origination above the ventricular tissue (in the atria).
Not all ventricular tachycardias are pulseless, and therefore, pulselessness must be established prior to beginning an algorithm. This is accomplished simply by checking a carotid or femoral pulse.
Pulselessness with a tachyarrhythmia occurs because the ventricles are not effectively moving blood out of the heart and there is, therefore, no cardiac output. Many tachyarrhythmias of a rate >150 will deteriorate into pulselessness if timely treatment is not given.
Pulseless ventricular tachycardia is treated using the left branch of the cardiac arrest algorithm. Click below to view the cardiac arrest algorithm diagram. When finished click again to close the diagram.
Cardiac Arrest Diagram

Click to view, and click again to close the diagram.
PALS Cardiac Arrest Diagram

Play the video below to see what a Pulseless Ventricular Tachycardia will generally look like on a defibrillator monitor. Allow several seconds for video to load. (4.03 mb)
Click for next Rhythm Review: Ventricular Fibrillation
Top Questions Asked on This Page
-
Q: What happens after the 2nd dose of Amiodarone is given and the patient is still in the same rhythm? Do we give a 3rd dose immediately or rhythm usually changes after 2nd dose?
A: A 3rd and even a 4th dose of 150 mg amiodarone may be administered. The only thing that needs to be taken into consideration is the 2.2-gram maximum dosage for 24 hours. Also, it is unlikely that the rhythm will remain VF or pVT long enough for you to get to the 3rd or 4th dose.
-
Q: What does refractory VT or VF mean?
A: Refractory pVT or VF means that the VF or pVT does not convert to a perfusing rhythm and continues to persist in spite of multiple attempts at conversion with defibrilation, acls drugs, and high quality CPR.
-
Q: After initiating CPR and assessing the rhythm, the patient is in VF/ pVT and the first shock is given, and CPR for 2 mins. Then rhythm check and in VT, should the pulse be checked to confirm pVT?
A: If there is no rhythm change and the same waveform of VT continues, you would not need to perform a pulse check. Performing the pulse check would delay the continuation of chest compressions. Once VT is pulseless it is very unlikely that any VT will be able to produce life-sustaining cardiac contractions.
lyonel says
I just stumbled over this site by accident , the wealth of information and the way it is formulated is amazing . Excellent job !!!!! Thank you.
Jessica Goode says
great help
Rosa M Strohbehn says
Good web side. I have the AHA manual and after I practice in your web side, I read my aha manual.
MaryAnn says
Hi,Jeff. You have under the PEA algorithm to shock if indicated. I thought PEA wasn’t shockable.
Jeff with admin. says
I could not find any reference to PEA on this page.
There is a common misunderstanding when referring to pulseless ventricular tachycardia. Some people think that pulseless ventricular tachycardia treated as PEA.
This is incorrect. Pulseless ventricular tachycardia is treated the same way that ventricular fibrillation is treated.
With unsynchronized high-energy shocks.
This is the left branch of the pulseless arrest algorithm.
PEA and asystole are treated using the right branch of the pulseless arrest algorithm.
Kind regards,
Jeff
Bruce Gustafson says
I’ve been taking ACLS since its inception, and this site is certainly more interesting for the purpose of reviewing, as compared to reading the book. I find the questions and feedback from other people not only educational, but also very interesting. Thanks for a great site!
Mebo says
am I correct in saying that “no pulse with any kind of arrhythmia” is PEA and if no pulse happens with ventricular tachycardia , then it is called pulseless ventricular tachycardia which is treated with cardioversion?
Jeff with admin. says
Basically, it is correct to say that any rhythm that does not have a pulse is PEA. Pulseless ventricular tachycardia and ventricular fibrillation are exceptions to how PEA is treated. Pulseless ventricular tachycardia and ventricular fibrillation are treated using The left branch of the pulseless arrest algorithm. This calls for unsynchronized shocks, otherwise known as defibrillation.
Kind regards,
Jeff
stephanie bray says
What, if any, are the early warning signs of pulsless ventricular tachycardia. Also can you elaborate more on the causes?
Jeff with admin. says
Major signs of VT which ultimately results in pulseless VT:
Chest pain, loss of consciousness, hypotension, chest pressure or tightness.
The most common cause of monomorphic ventricular tachycardia is myocardial scarring from a previous myocardial infarction (heart attack). This scar cannot conduct electrical current because of the dead tissue found along the electrical pathway. This can lead to a potential circuit around the scar that results in the ventricular tachycardia.
The most common cause of Polymorphic ventricular tachycardia is related to abnormalities of ventricular muscle repolarization. This is usually seen on the ECG as prolongation of the QT interval. QT prolongation may be congenital or acquired. One common congenital problem is Long QT syndrome. Acquired causes are usually related to drug toxicity or electrolyte abnormalities, but can be a result of myocardial ischemia. Some common drugs that may cause VT include some antibiotics and antihistamines, especially when they are used in combination with one another. Altered levels of potassium, magnesium and calcium can also cause VT.
Kind regards,
Jeff
becky12 says
This is my first time ever doing ACLS, Just become an EMT and wanting to go on – I love love love this site…….much better than all the books
ibrasebs says
Great site Jeff.
Makes things much easier than all other sites or books I have read.
Anny says
If ROSC, we transfer the patient to Post-Cardiac Arrest Care.
If no ROSC, when and how can we identify the patient is untreatable and stop CPR circles? Thanks!
Jeff with admin. says
First statement is correct. If ROSC then begin post cardiac arrest care.
Identifying when to stop CPR can be difficult. There is no set rule with this. It should be a team effort and the decision to stop CPR should be accomplished by team discussion and cooperation. All attempts to resuscitate the patient have failed and continued efforts seem to be in vain then stopping resuscitative efforts should be considered.
Kind regards,
Jeff
weetie33 says
This site is worth its weight in gold. I am using it to prepare for testing for a flight nurse position. The rhythm strips are great practice and the link to the medical university (i forgot the name) has extensive video instruction on EKG rhythms. Thank you!!
gerald says
is it PEA same mgt for assystole
Jeff with admin. says
Yes PEA and Asystole are managed the same. The right path of the Pulseless Arrest Algorithm should be used.
Kind regards,
Jeff
Brenda Biancosino says
The video shows Lidocaine as an option after Amiodarone…I thought Lidocaine was not an option anymore.
Jeff with admin. says
This page explains the standing of lidocaine within ACLS protocol: Lidocaine and ACLS
Kind regards,
Jeff
nabeel997 says
Yes lidocaine is not there in any algorithms 2010
Natalie says
I’ve been a RN for 10 years and have always dreaded taking ACLS until I found this wonderful website and all the tools it provides to assist any level of healthcare provider. THANKS
lawlorbill@yahoo.com says
What is the order of meds if we are shocking for 3rd, 4th and 5th time… etc, and can we give Epi and Amiodarone in same cycle of chest compressions…. thanks.. Bill
Jeff with admin. says
Once epinephrine has been started, it is given every 3-5 minutes on its own time table. It does not need to be coordinated with the chest compressions. It is just given every 3-5 minutes. The recorder should call out when it is due. Amiodarone has two doses in the algorithm 300mg and then 150mg if needed. There is no place for subsequent doses. The first dose of amiodarone is given after the 3rd shock and the 2nd dose of amiodarone is given at the earliest after the 4th shock. The main thing that you need to make sure of is that each medication has time to circulate before it is repeated. 2-4 minutes of high quality chest compressions should be sufficient to circulate a medication in to the system.
Epinephrine and amiodarone can be given in the same cycle of chest compressions.
Kind regards,
Jeff
Amanda says
Can we only give vasopressin once throughout the whole code and amiodarone twice throughout the whole code? Or is it when we find ourselves cycling back through the algorithm let’s say a third time we start out again as if we haven’t given vasopressin or amiodarone at all?
Jeff with admin. says
Yes, vasopressin is only given once. This is because the half life of vasopressin is around 20 minutes.
Amiodarone is usually given x 2 with one dose of 300mg and then a dose of 150mg. Usually pulseless VT/VF will not last long enough to give a third dose of 150mg, but it could be given if it was deemed necessary.
Kind regards,
Jeff