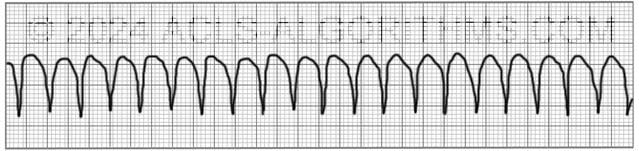
The pulseless ventricular tachycardia rhythm is primarily identified by several criteria. First, the rate is usually greater than 180 beats per minute, and the rhythm generally has a very wide QRS complex.
Second, the patient will be pulseless. And third, the rhythm originates in the ventricles. This is in contrast to other types of tachycardias which have origination above the ventricular tissue (in the atria).
Not all ventricular tachycardias are pulseless, and therefore, pulselessness must be established prior to beginning an algorithm. This is accomplished simply by checking a carotid or femoral pulse.
Pulselessness with a tachyarrhythmia occurs because the ventricles are not effectively moving blood out of the heart and there is, therefore, no cardiac output. Many tachyarrhythmias of a rate >150 will deteriorate into pulselessness if timely treatment is not given.
Pulseless ventricular tachycardia is treated using the left branch of the cardiac arrest algorithm. Click below to view the cardiac arrest algorithm diagram. When finished click again to close the diagram.
Cardiac Arrest Diagram

Click to view, and click again to close the diagram.
PALS Cardiac Arrest Diagram

Play the video below to see what a Pulseless Ventricular Tachycardia will generally look like on a defibrillator monitor. Allow several seconds for video to load. (4.03 mb)
Click for next Rhythm Review: Ventricular Fibrillation
Top Questions Asked on This Page
-
Q: What happens after the 2nd dose of Amiodarone is given and the patient is still in the same rhythm? Do we give a 3rd dose immediately or rhythm usually changes after 2nd dose?
A: A 3rd and even a 4th dose of 150 mg amiodarone may be administered. The only thing that needs to be taken into consideration is the 2.2-gram maximum dosage for 24 hours. Also, it is unlikely that the rhythm will remain VF or pVT long enough for you to get to the 3rd or 4th dose.
-
Q: What does refractory VT or VF mean?
A: Refractory pVT or VF means that the VF or pVT does not convert to a perfusing rhythm and continues to persist in spite of multiple attempts at conversion with defibrilation, acls drugs, and high quality CPR.
-
Q: After initiating CPR and assessing the rhythm, the patient is in VF/ pVT and the first shock is given, and CPR for 2 mins. Then rhythm check and in VT, should the pulse be checked to confirm pVT?
A: If there is no rhythm change and the same waveform of VT continues, you would not need to perform a pulse check. Performing the pulse check would delay the continuation of chest compressions. Once VT is pulseless it is very unlikely that any VT will be able to produce life-sustaining cardiac contractions.
pinkyrn says
Where is Right and Left in this diagram? Thanks
Jeff with admin. says
In the algorithm diagram, the VF/pulseless VT is the left branch and the PEA/Asystole is the right branch. I hope I am understanding your question correctly.
Kind regards,
Jeff
Steve says
This is fantastic!
I keep hearing different medical treatments for VT and VF. Is it possible for you to clarify once and for all the medications you would use, including dosages. Many thanks. Great site.
Jeff with admin. says
The American Heart Association has recommendations that are clearly laid out for first line medications. All of these drug interventions can be found here:ACLS medications.
You can also find more information on the treatment for pulseless ventricular tachycardia and ventricular fibrillation here:Ventricular fibrillation and pulseless ventricular tachycardia or.
Hope this helps.
Kind regards,
Jeff
Resmi Pillai says
hi jeff,
going for my first ACLS certification….very tensed…hoping for the best
resmi
Jeff with admin. says
You will do great! Good luck.
Kind regards, Jeff
Jeff with admin. says
You will do great! Good luck
Kind regards, Jeff
im1coolrn says
I won’t be taking ACLS without resubscribing to your site. This way of presenting the material makes it SO much easier to digest and remember. Thanks!
Jeff with admin. says
Thanks for the feedback. I’m so glad that it is helping. Kind regards, Jeff
GabrielMolina says
Hola
Estoy contento del ingreso a este servicio para compartir preguntas y experiencias de la capacitación, muy interesante y practico.
Jeff with admin. says
I’m so glad that the site is helpful for you. Kind regards, Jeff
yrrehSillenipS says
Every time I log on, this just gets better and better. I have been in critical care since 1999, and have always had a fear of not remembering the algorithms, especially the way they are represented in the AHA workbooks. These explanations are enabling me to put logic into each step of a code, rather than just rote memorization. Logic means increased memory retention for me.
Also, I appreciate that someone has spellchecked the material.
The best part is that I signed up for a year, so that after the test, I can continue to review things I haven’t used, but are bound to come up in some future code situation.
lkatminw says
I just registered onto this site and I am in awe of how resourceful it is. Reading the comment/responses section is helping answer my questions about algorithms. This is great! The responses are toned down,which is how I learn best. Thank you.
kcap says
Hello Jeff,
With the 1mg of Epinephrine, is that 1:1,000 or 1:10,000 dilution? Also, is the Epinephrine diluted prior to pushing the 1mg IV? Is it recommended to use Lidocaine as an antiarrhythmic, or is it more predictable to stick with Amiodarone?
Thank you,
K
Jeff with admin. says
Epinephrine vials are also labeled by concentration of a ratio of medication per mL.
CONCENTRATION
1:1,000=1mg/ml
1:10,000=0.1mg/ml
Most crash carts in the United States now come with pre-made 1:10,000 (1mg/10ml) syringes of epinephrine to help reduce the error of giving undiluted epinephrine. If you are using 1:1,000, you must dilute to 1:10,000 prior to administration for ACLS.
Amiodarone is the first-line antiarrhythmic for the cardiac arrest. Lidocaine can be used if amiodarone is not available.
Kind regards,
Jeff
ctruscott says
This is confusing regarding the dilution of Epi. You said if you are using Epi for ACLS, you must dilute to 1:10,000 which would equal 0.1 mg/ml. But the standard dose for Epi in V-Tach and V-Fib is 1 mg. Which is the correct dose then 0.1 mg/ml or 1mg/ml?
Thanks.
Jeff with admin. says
The correct dose would be to give 10ml of the 0.1mg/ml.
Kind regards,
Jeff
masoroti says
Will be my first time to take the AC LS. Just had a good feeling about this site.I like what users have to say about it!
Jeff with admin. says
Thank you for the feedback. I know you will do great with your first certification.
Kind regards, Jeff
Julie says
I think what MaryAnn was commiting on was on the Algorithm of PEA/Asystole it’s not a shockable, but didn’t understand once you give medication/CPR it can then become a shockable rhythm (where the yes and no arrows are).
Vanessa says
What would be the response someone would give having pulseless v-tach is occuring?
Jeff with admin. says
You should begin CPR and shock as soon as possible.
Kind regards,
Jeff
Jubilee01 says
very easy to understand thanks!
nissar says
How to differentiate between pulseless ventricular tachycardia and pulseless electrical activity?
Jeff with admin. says
PEA is an organized rhythm without a pulse except for VT.
Pulseless VT is in it’s one class and is treated in the same way as Ventricular Fibrillation.
Kind regards,
Jeff
Willard says
This is my second time using this site to prepare for my ACLS recertification. I find it very affordable, informative, user friendly, easy to navigate and understand. Thank you from the bottom of my Paramedic patch. Eng/PM Bill Mills
Jeff with admin. says
Thanks for the feedback and letting me know who your certification went. I am so glad that the site helped out. Kind regards, Jeff
Dr.Omar Nasif says
So great , it is really amazing site . Thanks alot