Atrial flutter is an abnormal heart rhythm that technically falls under the category of supra-ventricular tachycardias. Atrial flutter is typically not a stable rhythm and will frequently degenerate into atrial fibrillation.
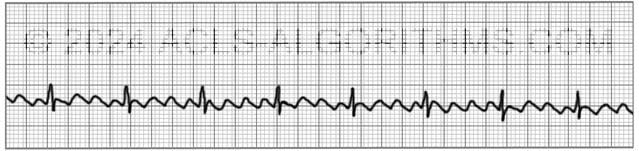
Atrial Flutter will usually present with atrial rates between 240-350 beats per minute. These rapid atrial rates are caused by electrical activity that moves in a self-perpetuating loop within the atria.
The impact and symptoms of atrial flutter depend upon the ventricular rate of the patient (i.e. cardiac output). Usually, with atrial flutter, not all of the atrial impulses will be conducted to the ventricles, and the more atrial impulses that are conducted, the greater the negative effect.
Symptoms
Symptoms of atrial flutter are similar to those of atrial fibrillation and may include the following:
- palpitations, chest pain or discomfort
- shortness of air
- lightheadedness or dizziness
- nausea
- nervousness and feelings of impending doom
- symptoms of heart failure such as activity intolerance and swelling of the legs occur with prolonged fast flutter)
Complications
As with its symptoms, atrial flutter shares the same complications as atrial fibrillation. These complications are usually due to ineffective atrial contractions and rapid ventricular rates. Ineffective atrial contractions can lead to thrombus formation in the atria and rapid ventricular rates can cause decompensation and heart failure.
Prevent complications from atrial flutter with early cardioversion.
Treatment
For the purposes of ACLS, atrial flutter is treated the same as atrial fibrillation. When atrial flutter produces hemodynamic instability and serious signs and symptoms, it is treated using ACLS protocol.
For the patient with unstable tachycardia due to this tachyarrhythmia (atrial flutter), immediate cardioversion is recommended. Drugs are not used to manage unstable tachycardia.
Cardioversion
Atrial flutter is considerably more sensitive to electrical direct-current cardioversion than atrial fibrillation, and usually requires a lower energy shock. 20-50J is commonly enough to revert to sinus rhythm.
AHA recommends an initial shock dose 0f 50-100 J for cardioverting unstable atrial flutter.
Below is a short video which will help you quickly identify atrial flutter on a monitor.
Please allow several seconds for the video to load. (3.84 mb)
Click for next Rhythm Review: Atrial Fibrillation
Questions Asked On This Page
-
Q: What are the chances of the formation of thrombus in the atrial cavity in the case of long-standing atrial flutter? Do we have to give anticoagulation, as in atrial fibrillation, to minimize the risk of emboli?
A: The chances for thrombus formation are relatively high. You would want to perform a TEE to ensure that there is no thrombus formation and you would want to initiate anticoagulation therapy.
-
Q: Energy levels for cardioversion of unstable a-flutter with both biphasic and monophasic devices? I haven’t seen anything as low as 20-50 joules mentioned in the AHA material, but I’m just getting started.
A: Unstable atrial flutter is treated as an unstable tachycardia within the tachycardia algorithm. Synchronized cardioversion is indicated, and the starting dose for narrow, regular tachycardia would be 50 J.
The page which states that 20-50 J can is used for the conversion of atrial flutter is speaking about atrial flutter in general and this could mean both stable and unstable atrial flutter.
Studies have shown that lower doses between 20-50 J are adequate for the conversion of atrial flutter. -
Q: I would assume that atrial flutter always has a rate more than 240. Are there any other rhythms that have rates that high? If not that might be one way to help identify flutter when not a sawtooth pattern.
A: Atrial flutter does not always have such a high atrial rate, but it usually will. Remember that flutter will many times only affect the atrial rate.
The ventricular rate may still be relatively low but usually more than 100. Symptoms will be seen when the ventricular rate is affected or if the patient develops a blood clot due to the pooling of blood in the atria related to the ineffective fluttering.
VT can have rates more than 240 but in this situation, the patient will most likely be pulseless, and you will treat using the cardiac arrest algorithm.
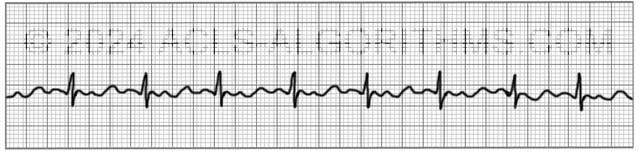
Usually, you will recognize atrial flutter by consistent saw-tooth or wave-like pattern between the QRS complexes.
amansard says
Where are the videos? There was only one.
Jeff with admin. says
If you watch the video on the home page, it will explain where the videos are found on the site. Kind regards, Jeff
tinkerbell says
hey—
what the heck is the F wave you elude to in the ACLS algorithm video. I am thinking that it is a mis-type and should be P. i am sure that i am not the only one that noticed this. thanks for correcting.
Jeff with admin. says
F-wave simply means “flutter” wave. This is the flutter wave that is seen with each electrical impulse of the atrial flutter.
Kind regards,
Jeff
chichi says
Hi …I have read about ECG in my accident and emergency course but my problem is that I seem not to understand how to interpretation it ….The stable tachycardia n unstable tachycardias….i really want to understand
Jeff with admin. says
Unstable tachycardia exists if a tachycardia is causing serious signs and symptoms in a patient. These serious signs and symptoms are related to poor blood perfusion.
Stable tachycardia exists if the patient has a tachycardia rhythm but continues to have good blood perfusion. I hope this answers your question.
Kind regards,
Jeff
Elaine12 says
I had an aha moment with the regular rate (a-flutter) and the irregular rate (a-fib) now on the video I can see the difference. Thank you.
Kathy gee says
“20-50J is commonly enough to revert to sinus rhythm.” but
“AHA recommends an initial shock dose 0f 50-100 J for cardioverting unstable atrial flutter.”
What dose is used for a flutter ?
When should you use the lower amount?
Thank you
Jeff with admin. says
The shock dose that American Heart Association recommends is 50 to 100 Joules.
There are times when expert cardiologist will use lower shock doses in certain situations. These lower shock deuces are typically reserved for experts who are very familiar with cardiac physiology.
Kind regards,
Jeff
rioboy10 says
2 quick questions….
In reference to A-Fib/A-Flutter (Stable), is the treatment to provide supplementary care (02, IV, Monitor, Pulse Ox, etc.) only and no Vagal Maneuvers and/or Adenosine 6mg/12mg IV?
Also, in ACLS, is the treatment for A-Fib/A-Flutter only in unstable pts?, which we would then go to synchronized cardioversion?
I just want to make sure that I fully understand the treatment modalities for stable A-Fib/A-Flutter because in the manual (AHA pg. 165), it states that Adenosine does not convert A-Fib and A-Flutter.
Thanks in advance for the help……this is a great site.
rioboy10 says
In simpler terms…..
In cases where the A-Fib and A-Flutter is “stable”, do we monitor the pt. only? and only treat A-Fib and A-Flutter if the pt. is deemed to be unstable?
Thanks again,
Jeff with admin. says
For stable atrial fibrillation and atrial flutter (new onset) monitoring the patient and the other interventions that you mentioned would be important, but you would also be looking for causes, consulting cardiology, and possibly using medications, like calcium channel blockers, to slow a rapid rate down. These other interventions for stable a-fib and a-flutter are important.
For the patient with any type of new onset atrial fibrillation (stable or unstable) it is important to rule out thrombus before a cardioversion is performed.
Kind regards,
Jeff
leilarocks says
How would you rule out the thrombus in the unstable patient before cardioversion? You wouldnt wait to do a CT or get back a D-dimer for the unstable patient would you?
(Aboslutely love this site btw!!)
Jeff with admin. says
Thanks for the compliment!
You would use an ultrasound procedure at the bedside that is called TEE Transesophageal echocardiogram. This procedure can be done rapidly at the bedside. If TEE is not available then the patient should be transferred to a facility where this procedure can be quickly done.
Kind regards,
Jeff
David says
the page says that drugs are not used to manage unstable tachycardia but wouldn’t adenosine be used if cardioversion failed to convert the patient?
David says
I was just hopping around the site, which is great by the way, but I may have misread the first time. It’s just the irregular unstable tachy rhythms that wouldn’t be treated with adenosine at all right?
Jeff with admin. says
Not exactly correct, but close. You would treat any unstable tachycardia with adenosine. You would go straight to cardioversion in all cases of unstable tachycardia where there is no underlying cause like sepsis. I’m talking about rates that will typically exceed 150 and most likely greater than 170.
Kind regards,
Jeff
Jeff with admin. says
I have never seen adenosine used after cardioversion when treating unstable tachycardia.
Amiodarone would probably be a better choice especially when dealing with wide complex tachycardia.
Kind regards,
Jeff
nagsen gajbhiye says
Very valuable information with video… its provide lot of help to recognize the atrial flutter
levy says
reliable website. all truth. thank you! learning in easy way
Btakahama says
atrial flutter video: what is F waves? the fluttering waves??
Jeff with admin. says
Correct. The atrial flutter waves are sometimes called F-waves.
Kind regards,
Jeff
obiking says
FYI on Chidi’s earlier comment.
Objective assesment of Nigerian’s heath care delivery system show, there has not been a concerted effort to organize an effective Emergency response system. Emergency Medicine exist only in Teaching hospitals and few large hospitals in Abuja, Lagos and Port-harcourt.
Therefore ACLS, ATLS and PALS are not emphasised tools of medical education for doctors even in very ‘sophisticated’ Hospitals.
Nigeria is far behind Ghana, South Africa, Egypt and perhaps Morrocco in entrenching the modicum of quality emergency services.
My experience is that doctors are still in ‘dark ages’ regarding these simple tools. A woman who collapsed in a bathroom, diaphoretic and hypotensive and obviously dypneic was given a ‘drip of Aminophylline and hydrocortisone, while an ER nurse was wrestling with the connectors of a nebulizer. This happened in the Emergency department of Umuahia ( A level 2 hospital by USA designation, and a teaching facility).
I was so flabbergatsed when I was informed that the doctor put the cause of death as ‘Status Astmaticus’
This happened to be my mum.
She had TIA a year prior and was treated in USA. She had just gone down to Nigeria from USA for her grand daughters wedding.
She obviously had either a PE or MI.
She had been ’embalmed by the time I flew back.
No autopsy.
there was no ECG done from my recollection, No CXR, No blood works (even if results came back post mortem)
That is Nigeria.
I am an ER physician, but in PEM.
I am hoping as a 50th birthday gift next year to design an emergency response protocal for the same town my mother died and use it a pilot for the country. I am currently looking for volunteer Er physicians to laise with me to do the paperwork. And possibly visit (after the Ebola scare) hopefully in Oct 2015.
Town population is maybe 1.5 million
One large facility about 100 bed. They have 3 health centers with urgent care facilities
They have oil money that can build an entire fleet of at least 10-15 equiped EMS ambulances and a dedicated emergency department built with a radio post.
With 90% penetrance of cellular phones in the general population, the idea of training young intelligent men and women as EMTs will not be difficult. Also simultanously train trainers and Physicians (who ever work in their ERs).
it is a dream.
It will be worth my while, if I can get a financial backbone.
Jim says
Hey Jim I Had almost similar experience last time I was in africa…chk out and may be join http://www.IMPII.org we can help you with what you trying to do.
asadullah buriro says
Axis
chidi says
I had been a cna, monitor tech and a nursing student. I also worked in a telemetry unit for over 5 years. though am in Africa at the moment, I really enjoyed the lessons and I miss working in the US so much. Nurses in Africa don’t have to go through ACLS. Can you guys imagine that?? Anyway, thank you so much Jeff. you are great. THANKS
Jeff with admin. says
So glad you are enjoying the site. Thanks for commenting. Kind regards, Jeff
Paul says
CHIDI, if nurses in NIGERIA don’t go through ACLS, don’t say that nurses in Africa don’t do ACLS!
NIGERIA IS NOT AFRICA ! Nigeria is just a country/state in Africa; and not an exemplary one for that matter.
Just as US of America is NOT THE CONTINENTOF NORTH AMERICA. USA is not the only country in AMERICA.
Travel to other AFRICAN countries – Egypt, South Africa, Morocco, Cameroun, Ethiopia, Ghana, etc; etc; and see what they are doing. Nursing is a universal science and abides to international standards.
Jeff, your classes are appreciated and used all over AFRICA !
GOD BLESS YOU.!
Paul; RN.
Pat says
Thank you Paul. That is the truth. ACLS is observed all over the world including NIGERIA. I don’t know where Chidi is speaking from. He really need to get more education about what he is talking about. Being a cna for several years and working in Tele unit for 5 years is not enough for Chidi to understand what ACLS entails.
Thanks again.
Pat. RN/BSN.
vu1nguyen says
what are F waves in atrial flutter? never heard of F waves before
Jeff with admin. says
Here is the medical dictionary definition for F waves.
F-waves: A pattern of regular, rapid atrial waves in an electrocardiogram, indicative of atrial flutter.
f-waves: A pattern of irregular undulations of the base line in an electrocardiogram that is indicative of atrial fibrillation.
Kind regards,
Jeff
Jeff with admin. says
This might make it a little more clear:
With atrial flutter, P waves are replaced by “F” waves (saw tooth pattern in II, III, AVF)
The F-waves are just a simple way to describe the electrical activity that moves in a localized self-perpetuating loop. For each cycle around the loop, there results an electric impulse that propagates through the atria.
This is in contrast to the P-wave which is a single impulse that discharges in the atria and initiates the QRS complex.
kellyQ says
Hi, so if I noticed my stable pt had an atrial flutter rate in the high 200s and a vent.rate in the 70s, would I follow the Adult Tachycardia w/ pulse Algorithm (pg.118)?
I see while traveling thru the Algorithm, I would end up at box 7 and if vagal maneuvers did not work, then Adenosine 6mg IV push would be given. Then I see on pg.165 under Adenosine Indications that: Adenosine does not convert atrial fibrillation, atrial flutter, or VT.
How do I treat sawtooth atrial flutter or do I need a cardiologist?
Jeff with admin. says
If the ventricular rate was in the 70’s then this would not be tachycardia and it would not be treated with the adult tachycardia algorithm.
If this was a new onset atrial flutter, you would want this patient to be admitted and consulted with a cardiologist.
Now if you had atrial flutter with an atrial rate in the 200’s and the ventricular rate was around 120-180’s you would treat using the adult tachycardia algorithm and get a cardiologist to evaluate the patient as soon as possible.
The ventricular rate is what determines if you progress into the use of the tachycardia algorithm.
Kind regards,
Jeff