
The most common cardiac arrhythmia, atrial fibrillation, occurs when the normal electrical impulses that are generated by the SA node are overwhelmed by disorganized electrical impulses in the atria.
These disorganized impulses cause the muscles of the upper chambers of the heart to quiver (fibrillate) and this leads to the conduction of irregular impulses to the ventricles.
For ACLS, atrial fibrillation becomes a problem when the fibrillation produces a rapid heart rate which reduces cardiac output and causes symptoms or an unstable condition.
When atrial fibrillation occurs with a (RVR) rapid ventricular rate (rate > 100 beats/min), this is called a tachyarrhythmia. This tachyarrhythmia may or may not produce symptoms. Significant symptoms that occur are due to a reduction in cardiac output.

The following is a list of the most common symptoms.
- palpitations or chest discomfort
- shortness of air and possibly respiratory distress
- hypotension, light-headedness and possibly loss of consciousness
- peripheral edema, jugular vein distention, and possibly pulmonary edema
For the purpose of ACLS, it is important to be able to recognize atrial fibrillation when the patient is symptomatic. On an ECG monitor, there are two major characteristics that will help you identify atrial fibrillation.
- No p-waves before the QRS on the ECG. This is because there are no coordinated atrial contractions.
- The heart rate will be irregular. Irregular impulses that the ventricles are receiving cause the irregular heart rate.
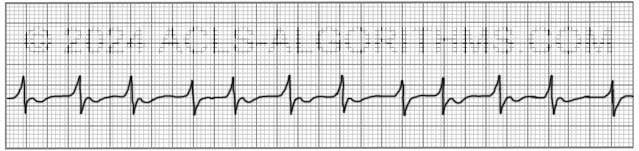
When the heart rate is extremely rapid, it may be difficult to determine if the rate is irregular, and the absence of p-waves will be the best indicator of atrial fibrillation.
ACLS Treatments:
For the purposes of ACLS atrial fibrillation is treated when the arrhythmia/tachyarrhythmia produces hemodynamic instability and serious signs and symptoms.
For the patient with unstable tachycardia due to a tachyarrhythmia, immediate cardioversion is recommended. Drugs are not used to manage unstable tachycardia. The appropriate voltage for cardioverting unstable atrial fibrillation is 120-200 J.
Cardioversion of stable atrial fibrillation should be performed with caution if the arrhythmia is more than 48 hours old and no anticoagulant therapy has been initiated due to the risk of emboli that can cause MI and stroke.
Below is a short video which will help you quickly identify atrial fibrillation on a monitor.
Please allow several seconds for the video to load. (5.11 mb)
Click for next Rhythm Review: Other Tachycardias
Top Questions Asked On This Page
-
Q: To treat a patient with rapid atrial fibrillation (HR >180bpm), can calcium channel blockers be given to help control the rate?
A: Yes, in some cases, calcium channel blockers are a good choice to help control atrial fibrillation with a rapid ventricular rate.
-
Q: What are atrial fibrillation and atrial flutter considered in terms of narrow or wide QRS complexes?
A: Unless there is an underlying block the QRS complex will typically be normal/narrow. There is the possibility of occasional wide QRS complexes due to abnormal ventricular depolarization via an accessory pathway.
-
Q: What does the DC before the word cardioversion stand for?
A: DC cardioversion simply means direct current cardioversion.
Mng1942 says
Very helpful site for me as a PCP.Thanks.Mani.
Mansab Amin says
excellent. good revion ,easy to remember .
Mansab Amin says
excellent. good revesion ,easy to remember .
Jalal says
Imagine a patient brought to ER with SBP <90, sweating and chest pain and ECG shows Atrial fibrillation. TEE is performed and Shows thrombus. What should be our line of treatment? Should we go for cardioversion or should we initiate anticoagulation before cardioversion?
Regards
Jalal
Jeff with admin. says
You would not want to use cardioversion with this patient at this time. The patient would probably be placed on some type of anticoagulant and given something to decrease the heart rate and possibly something to improve blood pressure.
This patient would need to be medically managed until the patient could be seen by a cardiologist.
Kind regards,
Jeff
slpatti says
Cardioversion begins at what level?
Jeff with admin. says
For the patient who has atrial fibrillation, the indication for cardioversion would be if the patient is hemodynamically unstable. Some things to look for would be SBP< 90mmhg, altered mental status, and chest pain.
Also, with atrial fibrillation a TEE (Transesophageal Echocardiogram) should be performed prior to cardioversion if the pt. has not had anticoagulant therapy. This would ensure that the patient did not have any type of thrombus that could worsen the patient’s condition if cardioversion is performed.
Kind regards,
Jeff
herb_wms says
I assume when you are say get TEE before cardioversion that in a stable patient?
Herb
Jeff with admin. says
Yes, this would be for a patient that is stable but symptomatic.
Kind regards,
Jeff
Yacob says
this site is save me from alot of missing during my lecture,,,, thank you alot
Ramki. says
what is the drug of choice for AF ? Here our cardiologists use Amiodarone regularly. Do we have to treart rate & rhythm seperately in AF ?.
Jeff with admin. says
I would not say that there is one drug of choice for atrial fibrillation.
In the critical care setting when atrial fibrillation is accompanied with a rapid ventricular rate amiodarone is used. Quite frequently, I have seen cardizem or some other calcium channel blocker used to slow the heart rate.
Kind regards,
Jeff
Ilecia says
Hi Jeff, I must say that I do love this site, it is helping me tremendously in preparing for ACLS coming up in the next 8 days.
What are some of the beta blockers that are used in the stable tachyarrhythmias?
Jeff with admin. says
Metoprolol, labetalol, and Propranalol are commonly used but there are others.
Kind regards,
Jeff
Mommaroz says
I think having a strip on top of all of the arrhythmia pages would be helpful. When I want to go back and forth between arrythmia’s to compare and figure out the difference in appearance I find it frustrating that I have to play the video for atrial fib to see a strip. Also if the videos had the capability to back up so you don’t have to replay the whole video when you don’t understand one little section that would be awesome. I seem to be having trouble recognizing atrial fib. Any hints? This site is great and has been extremely helpful. Thank you
Jeff with admin. says
There is as image up on this page now. Thanks for pointing this out. Remember this for a-fib: Irregular rate and no P-waves. If you see an irregular heart rate and no p-waves, there is a high likelihood that you are dealing atrial fibrillation.
Kind regards,
Jeff
SYED RAZA says
Why choose Verapamil ?
It depends if you are planning a rate control (option ) or rhythm control (not a good option) strategy.
Beta blockers are however considered to be superior as far as the negative chronotropic effect is concerned.
However, be careful if you are dealing with AF with pre-excitation i.e. WPW as using BB and Verapamil may be catastrophic,
Debra says
Your site and WONDERFUL FORMAT has SAVED ME from the American Heart ACLS book!
T H A N K Y O U!
Kathleen says
What are your thoughts on administering Verapamil in the pre hospital setting of AF?
Chris with admin. says
I can’t really comment on it, because I haven’t used it in the pre-hospital
setting. I performed a cursory literature search and could not find any
studies comparing verapamil with say amiodarone or synchronized
Cardioversion. I will look around a bit more and see what I can find.
Kind regards,
Chris
itsKevin says
Amiodarone seems to be a common choice among physicians for treating A-fib with RVR at the facility where I work. Giving a 150 mg bolus followed by a continueous infusion seems to do the trick. I can’t remember I time when this hasn’t worked for at least controlling the rate.
LynzeN84 says
I love this website, for the first time I feel like I will truly understand what is going on during a code, not just following instructions as a nurse. But I would like your opinion on something, I work on a cardiovascular step down unit and Im about to transition to the cardiovascular ICU, we work with CABG pts post op. We see A LOT of a-fib after surgery, do you think the electrial activity just gets “messed up” because of swelling of the heart? Not sure if I heard another medical professional tell a pt that or if honestly I just made it up in my head!! lol! Just wondering your opinion. And thanks again for this site, I will def recommend this site to my co-workers.
Jeff with admin. says
I can’t say that I have an opinion, but I did find some literature that might give some insight. Here is the link:
Here are a couple of quotes from the article that may shed some light on the subject:
“The precise mechanism of post-bypass AF is incompletely understood, and is still being investigated. In the predominantly elderly group of patients who undergo coronary bypass surgery, age-related structural changes such as atrial dilatation, hypertrophy, fibrosis and senile amyloidosis occur to varying degrees of severity in the atrium. This already heterogeneous myocardium, on being subjected to operative trauma and subsequent post-operative inflammation and edema, becomes a tissue mosaic of differing refractory periods and conduction velocities susceptible to aberrant electrical activity, conduction and re-entry – the ‘anisotropic’ atrium.
“In patients with an anisotropic atrium, AF may be triggered by post-operative pericarditis, autonomic imbalance, withdrawal of beta blockers, fluctuating electrolytes and blood gases. Two thirds of the post-bypass AF occurs on the second or third day: this correlates with the development of post-operative inflammatory pericarditis and the inflammatory infiltration of the myocardium[12] that increase the anisotropic nature of the atrium. The post-operative autonomic imbalance is believed to sensitize the myocardium to arrhythmogenic insults.[13-17] The electrophysiological characteristics of atrial cells, action potential duration, refractoriness and conduction speed are all modulated in opposing ways by vagal and sympathetic influences. High vagal tone favors macro reentry, while increase in sympathetic tone favors abnormal automaticity and triggered activity. Fluctuations in autonomic tone, with a primary increase in adrenergic drive followed by a marked shift towards vagal predominance, have been noted just before the onset of AF in some patients.”
Hope this helps.
Also thank you for the encouraging feedback.
Kind regards,
Jeff
RCavanaugh says
Love this site! Thanks!
Ruth
Susan Montani says
Jeff, do you know if Cardizem is a medical control drug in state of MA?
erinlfisk says
You can give Cardizem without medical control in MA for Afib/Aflutter. You obviously have to follow the standing orders which are if the patient is stable but symptomatic, and the heart rate is greater than 150, first dose .25mg/kg slow iv push over two minutes, then if in 15 minutes no change, can give the second dose at .35mg/kg slow iv push over two minutes. Protocols say if the heart rate is less than 150 then must contact medical control and if the second dose does not work. Just have to watch for people with WPW. Hope this helps. I just moved from MA to TN so have to learn a totally different way of thinking and freedom from medical control here aka most everything is standing order!
paguero says
Is sync-ing a-fib starting at 200j new this year, and sync-ing futter starting at 50j also new..?
Jeff with admin. says
Yes both of these are new. AHA states:
2010 (New): The recommended initial biphasic energy dose
for cardioversion of atrial fibrillation is 120 to 200 J.
Cardioversion of adult atrial flutter and other supraventricular
rhythms generally requires less energy; an initial energy of
50 to 100 J with either a monophasic or a biphasic device is
often sufficient.
From: Highlights of the 2010-2015 ACLS Guidelines
Kind regards,
Jeff