
The most common cardiac arrhythmia, atrial fibrillation, occurs when the normal electrical impulses that are generated by the SA node are overwhelmed by disorganized electrical impulses in the atria.
These disorganized impulses cause the muscles of the upper chambers of the heart to quiver (fibrillate) and this leads to the conduction of irregular impulses to the ventricles.
For ACLS, atrial fibrillation becomes a problem when the fibrillation produces a rapid heart rate which reduces cardiac output and causes symptoms or an unstable condition.
When atrial fibrillation occurs with a (RVR) rapid ventricular rate (rate > 100 beats/min), this is called a tachyarrhythmia. This tachyarrhythmia may or may not produce symptoms. Significant symptoms that occur are due to a reduction in cardiac output.

The following is a list of the most common symptoms.
- palpitations or chest discomfort
- shortness of air and possibly respiratory distress
- hypotension, light-headedness and possibly loss of consciousness
- peripheral edema, jugular vein distention, and possibly pulmonary edema
For the purpose of ACLS, it is important to be able to recognize atrial fibrillation when the patient is symptomatic. On an ECG monitor, there are two major characteristics that will help you identify atrial fibrillation.
- No p-waves before the QRS on the ECG. This is because there are no coordinated atrial contractions.
- The heart rate will be irregular. Irregular impulses that the ventricles are receiving cause the irregular heart rate.
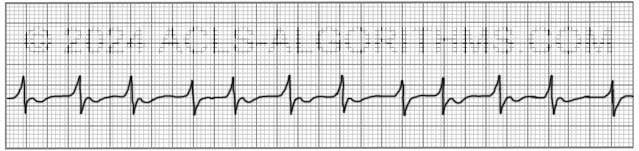
When the heart rate is extremely rapid, it may be difficult to determine if the rate is irregular, and the absence of p-waves will be the best indicator of atrial fibrillation.
ACLS Treatments:
For the purposes of ACLS atrial fibrillation is treated when the arrhythmia/tachyarrhythmia produces hemodynamic instability and serious signs and symptoms.
For the patient with unstable tachycardia due to a tachyarrhythmia, immediate cardioversion is recommended. Drugs are not used to manage unstable tachycardia. The appropriate voltage for cardioverting unstable atrial fibrillation is 120-200 J.
Cardioversion of stable atrial fibrillation should be performed with caution if the arrhythmia is more than 48 hours old and no anticoagulant therapy has been initiated due to the risk of emboli that can cause MI and stroke.
Below is a short video which will help you quickly identify atrial fibrillation on a monitor.
Please allow several seconds for the video to load. (5.11 mb)
Click for next Rhythm Review: Other Tachycardias
Top Questions Asked On This Page
-
Q: To treat a patient with rapid atrial fibrillation (HR >180bpm), can calcium channel blockers be given to help control the rate?
A: Yes, in some cases, calcium channel blockers are a good choice to help control atrial fibrillation with a rapid ventricular rate.
-
Q: What are atrial fibrillation and atrial flutter considered in terms of narrow or wide QRS complexes?
A: Unless there is an underlying block the QRS complex will typically be normal/narrow. There is the possibility of occasional wide QRS complexes due to abnormal ventricular depolarization via an accessory pathway.
-
Q: What does the DC before the word cardioversion stand for?
A: DC cardioversion simply means direct current cardioversion.
Barbara says
That’s great,the knowledge s so impressive from low to high level
walid says
thanks for this wonderful site
i cannot find an answer for this mcq
-35 year old morbidly obese patient is discharged after gastric bypass surgery. She is readmitted 4 days later after she falls and twists her ankle. She is noted in the ER to be in atrial fibrillation, she is hypotensive, but only complains of leg pain. She is admitted to the hospital and temperature on admission is 38.6 c and heart rate 105.
The next step in the management of her dysrythmia should be
a- Ibutilide
b- Procainamide
c- Echocardiographic study
d- DC cardioversion
e- Digitalis
Jeff with admin. says
The answer would be “C” the next step would be an echocardiographic study. This is because you would want to ensure that the atrial fibrillation did not cause any clots to form in the heart. Once thrombus is ruled out, you are ok to perform cardioversion if necessary.
When a person has new onset atrial fibrillation, it can cause a thrombus to form in the heart and this can lead to a life threatening problem. This is why it is important to get an echocardiographic study completed as soon as possible.
Kind regards,
Jeff
Codehanadi says
Thank you
cdfrick says
Hi Jeff –
What is the recommendation level of electrical shock – Cardio Version – with atrial fib? Same as with A-flutter?
Jeff with admin. says
Here are the cardioversion voltage doses:
Pg. 118: “Initial recommended doses:
-narrow regular: 50-100 J
-Narrow irregular: 120-200 J biphasic or 200 J monophasic
-Wide regular: 100 J
-Wide irregular: defibrillation dose (not synchronized)”
Kind regards,
Jeff
Md Islam says
Hi Jeff
What is the 2nd line of Rx of stable AF with rapid ventricular ,not responding to beta blocker or Calcium channel blocker +/- digoxin. Can we use amiodarone for rate control even if AF persisting more than 48 hr ?
Jeff with admin. says
Management of atrial fibrillation is complex and treatments can vary depending on duration of atrial fibrillation, co-morbidities, underlying cause, symptoms, and age. Here is a link to an AHA PDF on the guidelines for treating Atrial Fibrillation.
Kind regards,
Jeff
Eric Beason says
Is NGT contraindicated in rapid AF with associated angina due to preload and afterload being possibly compromised?
Jeff with admin. says
If the angina is being caused by the rapid AF, then NTG (nitroglycerine) would not be indicated. You would want to deal with the rapid heart rate. Deal with the rapid rate and you will most likely relief the angina. A drop in pressure related to the NTG could further compromise the patient’s already compromised perfusion. Kind regards, Jeff
heymicks says
Hi, in hospital setting, noted that diltiazem IVP is administered attempting to convert afib/atrial flutter. It does convert to sinus rhythm for some time but then it recurrs. I observed one patient, it recurs for 4 nights consecutively but it converted once dilt was given, but then finally was transferred to med-tele unit for a dilt drip due to its recurrence at night. Is diltiazem part of ACLS cardiac meds with afib? Hemodynamically, pt is really on low side, low hct of 22 (had transfusion), low platelet of 12,000, low wbc 700 s/p stem cell transplant. Pt’s symptoms were fatigue and fever.
Jeff with admin. says
Diltiazem is not part of basic ACLS protocol. However, advanced ACLS protocol does include the use of diltiazem.
In light of the situation that you mention, there is a very good possibility that the afib was related to patient’s medical condition. Fever, fatigue, low WBC, low hct are symptoms that something is going wrong in the body.
Whatever was wrong could have likely been causing irritability to the heart. This irritability could have caused the atrial fibrillation.
It would be important to correct any underlying conditions that could be exacerbating the atrial fibrillation. After correcting these problems then you would address the atrial fibrillation.
Kind regards,
Jeff
Jasmin says
Hello Jeff. I will be taking my ACLS class in about three weeks and I just want you to know how invaluable this information is for me right now. I have been a nurse for three years and have worked med-surg/tele my entire career. The funny part about that is I have had no training (aside from nursing school) regarding ECG and rhythm interpretation, so you can imagine how exciting this all is for me. Your format is just the best I have seen and I am now truly starting to understand this oh so important information.
However I do have one question, and this is more of just a clarification. With new and unstable Afib or Aflutter, immediate cardioversion is indicated, correct?? And this is regardless of any anticoagulation being on board or TEE being performed, correct?? I wanted to clarify of course for ACLS but also for real life situations, as I’ve never witnessed a patient with unstable Afib or Aflutter requiring synchronized cardioversion. Thanks again!
Jeff with admin. says
You would want to perform a TEE prior to synchronized cardioversion or at least clear the cardioversion with a cardiologist prior to synchronized cardioversion. I have had symptomatic patient with afib and aflutter, but we never had to resort to immediate cardioversion.
Kind regards,
Jeff
John says
What is better in treatment of atrial arrythmia verapamil or pindolol?
Jeff with admin. says
I do not have enough background to answer this question, but this research article may shed some light for you. Kind regards, Jeff
odessa1a says
I have a stupid question. If a patient has one of the symptoms listed does this make them unstable or would there need to be changes in vital signs also.
Jeff with admin. says
You would see a change in vital signs that would be related to poor perfusion. You would also consider serious signs and symptoms as unstable. The most common of these s/s are: chest pain, signs of shock, SOA, altered mental status, weakness, fatigue, and syncope.
Kind regards,
Jeff
janaka says
Short video is useful to identify AF during resuscitation of patient. Actually it is a practical guide for ACLS
LILLYROSE222 says
This site is brilliant. How, though, to treat symptomatic bradycardia with afib? Atropine and pacing?
Jeff with admin. says
It depends if the atrial fibrillation is new onset. If it is new onset then it should be taken care of after the patient is stabilized and the cause of the bradycardia dealt with. Treat the patients slow rate first. Pacing would probably be the easiest intervention that would stabilize the patient. ECG and cardiac enzymes should be checked to r/o myocardial infarction.
Kind regards,
Jeff
shweta garg says
Hello Jeff,
I had a question about a fib. Suppose a patient has new onset a fib. and unstable with SBP of 80. and they have clear sepsis with lactate of 4. Would you cardiovert or give fluids first ?
Jeff with admin. says
I would give fluids first. It is very likely that the hypotension is related to sepsis rather than the atrial fibrillation. You can give 500-1000 ml of fluid fairly rapidly to determine if the patient will stabilize.
Also, if the duration of being in atrial fibrillation is not known, then a TEE (Trans-esophageal Echocardiogram) would need to be performed to rule out thrombosis prior to any thought of cardioversion.
Kind regards,
Jeff
Argo says
Hi,
The video and your website are great. About shocks,how much do you use in acute A fib? 120 J? What do you give for sedation? Do you use any benzodiazepines?
Thanks in advance,
Jeff with admin. says
Acute unstable a-fib would present as a narrow irregular tachycardia. This is treated with a starting dose of 120-200 J synchronized cardioversion. You would use some form of sedation.
Kind regards,
Jeff
pjbrant says
I do appreciate your training that mentions a big caution in cardioversion in atrial fib & atrial flutter for those patients that have presumably who have been living with their symptoms for awhile (over 48 hrs) knowingly or unknowingly, WITHOUT the benefit of anticoagulation or TEEs to verify thrombus formation or not. Your information suggests holding off on cardioversion until heparin IV drip or other effective anti-coagulant treatment for potential thrombus has occurred.
I have searched the AHA manual ( 2011 printing) and do not see any training on this. Please correct me if I’m missing some important information. But I would like to be prepared for the expectation in real life for this “red-flag” or at least be prepared if it is a current AHA training point or not.- maybe to see in a test question or scenario?
Jeff with admin. says
The information that was discussed about TEE to rule out thrombus is a little beyond the scope of basic ACLS, and it is why you did not find in in the ACLS provider manual. The treatment of afib or aflutter that has gone untreated beyond 48 hours (or unknown) will probably not come up ACLS class or in testing.
Also, the only place where this is discussed on the site is in the comments. This is because the question has been brought up several times by other students on the site.
It is highly unlikely that you will discuss this in ACLS Class, but it is a very important bit of information to retain.
Kind regards,
Jeff