
The most common cardiac arrhythmia, atrial fibrillation, occurs when the normal electrical impulses that are generated by the SA node are overwhelmed by disorganized electrical impulses in the atria.
These disorganized impulses cause the muscles of the upper chambers of the heart to quiver (fibrillate) and this leads to the conduction of irregular impulses to the ventricles.
For ACLS, atrial fibrillation becomes a problem when the fibrillation produces a rapid heart rate which reduces cardiac output and causes symptoms or an unstable condition.
When atrial fibrillation occurs with a (RVR) rapid ventricular rate (rate > 100 beats/min), this is called a tachyarrhythmia. This tachyarrhythmia may or may not produce symptoms. Significant symptoms that occur are due to a reduction in cardiac output.

The following is a list of the most common symptoms.
- palpitations or chest discomfort
- shortness of air and possibly respiratory distress
- hypotension, light-headedness and possibly loss of consciousness
- peripheral edema, jugular vein distention, and possibly pulmonary edema
For the purpose of ACLS, it is important to be able to recognize atrial fibrillation when the patient is symptomatic. On an ECG monitor, there are two major characteristics that will help you identify atrial fibrillation.
- No p-waves before the QRS on the ECG. This is because there are no coordinated atrial contractions.
- The heart rate will be irregular. Irregular impulses that the ventricles are receiving cause the irregular heart rate.
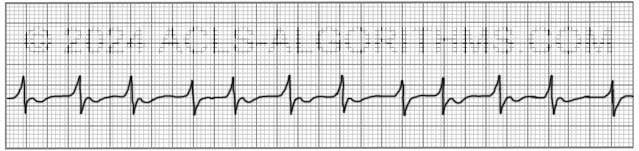
When the heart rate is extremely rapid, it may be difficult to determine if the rate is irregular, and the absence of p-waves will be the best indicator of atrial fibrillation.
ACLS Treatments:
For the purposes of ACLS atrial fibrillation is treated when the arrhythmia/tachyarrhythmia produces hemodynamic instability and serious signs and symptoms.
For the patient with unstable tachycardia due to a tachyarrhythmia, immediate cardioversion is recommended. Drugs are not used to manage unstable tachycardia. The appropriate voltage for cardioverting unstable atrial fibrillation is 120-200 J.
Cardioversion of stable atrial fibrillation should be performed with caution if the arrhythmia is more than 48 hours old and no anticoagulant therapy has been initiated due to the risk of emboli that can cause MI and stroke.
Below is a short video which will help you quickly identify atrial fibrillation on a monitor.
Please allow several seconds for the video to load. (5.11 mb)
Click for next Rhythm Review: Other Tachycardias
Top Questions Asked On This Page
-
Q: To treat a patient with rapid atrial fibrillation (HR >180bpm), can calcium channel blockers be given to help control the rate?
A: Yes, in some cases, calcium channel blockers are a good choice to help control atrial fibrillation with a rapid ventricular rate.
-
Q: What are atrial fibrillation and atrial flutter considered in terms of narrow or wide QRS complexes?
A: Unless there is an underlying block the QRS complex will typically be normal/narrow. There is the possibility of occasional wide QRS complexes due to abnormal ventricular depolarization via an accessory pathway.
-
Q: What does the DC before the word cardioversion stand for?
A: DC cardioversion simply means direct current cardioversion.