Ventricular fibrillation (VF) occurs when there are uncoordinated contractions within the ventricles of the heart. The primary cause of VF is hypoxia (lack of oxygen) to the heart muscle, which causes hyperirritability in the cardiac muscle tissue.
As a result, multiple muscle cells within the ventricles simultaneously fire as pacemakers causing a quivering or fibrillation that is ineffective for adequate cardiac output.
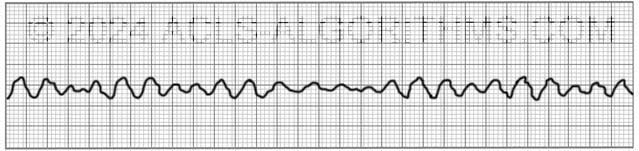
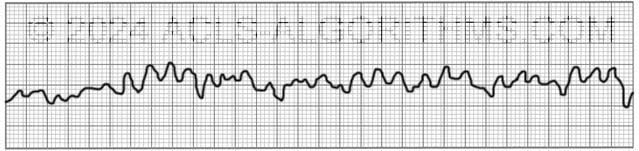
The two images show what ventricular fibrillation will look like on an EKG rhythm strip.
VF can rapidly lead to heart muscle ischemia, and there is a high likelihood that it will deteriorate into asystole.
Ventricular fibrillation is treated using the left branch of the cardiac arrest algorithm. Click below to view the cardiac arrest algorithm diagram. When done click again to close the diagram.
Cardiac Arrest Diagram

Click to view, and click again to close the diagram.
PALS Cardiac Arrest Diagram

Ventricular fibrillation is always pulseless and must be confirmed by EKG or defibrillator monitor. Defibrillation is the treatment of choice and should occur as soon as possible.
The video below shows an example of what ventricular fibrillation will look like when you see it on the defibrillator monitor. Please allow several seconds for the video to load. (7.24mb)
Click for next Rhythm Review: Pulseless Electrical Activity
Top Questions Asked on This Page
-
Q: Why does it say VFib is always pulseless? My thinking is an organized rhythm with no pulse will be PEA, then should be treated as on R branch of the cardiac arrest algorithm.
A: Ventricular fibrillation is not an organized rhythm. It is a chaotic and disorganized rhythm. There is no organization to the rhythm. There are no p-waves and no QRS complexes.
-
Q: Which concentration of Lidocaine is given intravenously in ACLS considering that there is the local anesthetic as well. Is the 2% safe?
A: Typically, lidocaine for IV infusion is mixed 2000 mg lidocaine in 500 ml. This works out to a 4 mg/ml dilution.
Two percent lidocaine is a 20 mg/ml. This 20 mg/ml would need to be diluted to obtain the 4 mg/ml dilution.
You would not want to give 2% lidocaine without diluting to 4 mg/ml. The main reason for dilution is to avoid rapid high plasma concentrations and reduce toxicity risk -
Q: When does the sodium bicarb injection need to be administered and when does the lidocaine IV need to be administered?
A: Here is the AHA position on Sodium Bicarbonate:
“In some special resuscitation situations, such as preexisting metabolic acidosis, hyperkalemia, or tricyclic antidepressant overdose, bicarbonate can be beneficial (see Part 10: Special Circumstances of Resuscitation).
However, routine use of sodium bicarbonate is not recommended for patients in cardiac arrest.”
Here is the AHA position for Lidocaine:
“There is inadequate evidence to support the routine use of lidocaine after cardiac arrest. However, the initiation or continuation of lidocaine may be considered immediately after ROSC from cardiac arrest due to VF/pVT.
Lidocaine may be considered as an alternative to amiodarone for VF/pVT that is unresponsive to CPR, defibrillation, and vasopressor therapy.
rsbdlps says
I’m sure the initiation of oxygen is implied at the beginning of the algorithm with the initiation of CPR. Love this site
Jeff with admin. says
In the algorithm diagram on this page, application of oxygen is shown in the top blue box. If I you happen notice some places on the site where it is not mentioned (application of oxygen) and should be, kindly let me know and I will get it added in. —Kind regards, Jeff
nurserachelbethel says
I have worked in ambulatory surgery and vascular pre and post surgery for years. A new
job is requiring acls certification. Identifying and treating cardiac rhythms has not been part
of my practice! This web site has been so helpful. Seeing the rhythms on the screen with
practice sessions have adequately prepared me for my class. Thankyou for the excellent
site!
Ruth Cloud says
This information is most helpfull to me preparing for ACLS re-certerfication.
I can study at home at my convenience.
Thank you so much. I will inform my friends at work.
Lee says
Just a little comment, according to AHA, PEA is non shockable while VT/VF are shockable. Therefore, VF should not follow PEA algorithm =) It should follow the same algorithm as pulseless VT
Jeff with admin. says
That is correct.
Vibha says
Very useful and precise information .Thank you
larry r hill says
wow, I really needed thius info
Donna Prochaska says
I have been a nurse for years, and am taking the ACLS course for the second time in two years. You have to know your rhythms first, and I wish I had known of this site the first time.
Zahidullah Khan says
Great work and great site
Holly Tays says
thanks
Olive Green says
I will be doing my ACLS in October, glad I’ve found this site!
Elaine McKinney says
Good to be able to see the rhythms in action.Can play over and over until you understand
belle says
I will have my Megacode practical test on august 20. Glad I found your website it is helpful for my preparation for the Megacode I hope I will pass the test… Thanks
reggie says
Love, love this site.
mardiana says
i like dis channel…hope i can past my acls course..
barbara says
I love this website. Decreases my worry on passing Megacode in ACLS. I work on OB and do not regularly work with heart rhythms. I hope I will pass tomorrow. Thanks