Second degree heart block Type 2, which is also called Mobitz II or Hay, is a disease of the electrical conduction system of the heart. Second-degree AV block (Type 2) is almost always a disease of the distal conduction system located in the ventricular portion of the myocardium.
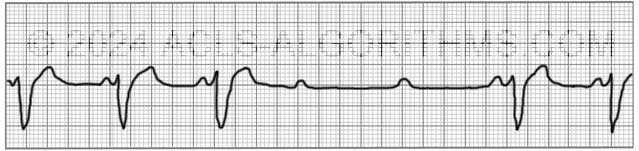
This rhythm can be recognized by the following characteristics:
- non-conducted p-waves (electrical impulse conducts through the AV node but complete conduction through the ventricles is blocked, thus no QRS)
- P-waves are not preceded by PR prolongation as with second-degree AV block (Type 1)
- fixed PR interval
- The QRS complex will likely be wide
Click here to see why.
The QRS on an ECG will most likely be wide because the block occurs in the His bundle or bundle branches and conduction through the ventricles is slowed. This slowing of conduction appears as a wide QRS complex on the ECG.

Second-degree heart block type 2 is usually caused by structural damage to the conduction system of the heart. Causes of the structural damage to the conduction system include the following:
Causes:
- Myocardial infarction that damages the conduction system
- Idiopathic fibrosis
- Cardiac surgery
- Infections and inflammatory conditions
- Hyperkalemia
- Autoimmune diseases affecting the heart
Second-degree AV block (Type 2) should be treated with immediate transcutaneous pacing or transvenous pacing because there is risk that electrical impulses will not be able to reach the ventricles and produce ventricular contraction.
Second-degree AV block (Type 2) is clinically significant because this rhythm can rapidly progress to complete heart block.
Atropine may be attempted if immediate TCP is not available or time is needed to initiate TCP. Atropine should not be relied upon and in the case of myocardial ischemia it should be avoided.
Below is a short video which will help you quickly identify second-degree heart block type 2 on a monitor. Please allow several seconds for the video to load. (2.65 mb)
Click for next Rhythm Review:
Complete Heart Block (3rd Degree Block)
Top Questions Asked On This Page
-
Q: The video says “sometimes has wide QRS.” What else would you see with 2nd-degree if the block is occurring in the bundled His? I have seen the portrayed rhythm many times and was not sure what it was.
A: For 2nd-degree block type II you will see:
non-conducted p-waves (electrical impulse conducts through the AV node, but complete conduction through the ventricles is blocked, thus no QRS)
P-waves are not preceded by PR prolongation as with second-degree AV block (Type 1)
fixed PR interval -
Q: Having trouble differentiating between Mobitz II and third-degree block.
A: The main difference is this:
Mobitz II: There will be a P-wave with every QRS. There may not always be a QRS complex with every p-wave. The rate will usually be regular. Also, the PR interval will be regular.
3rd Degree Block: There may not be a p-wave with each QRS, and the PR interval will not be the same with each PQRS.
These videos may help you.
They are kind of hard to hear, but the content is good. -
Q: Your video says pace right away for 2nd degree? TCP should only take place if the patient is symptomatic or showing signs of inadequate perfusion? Correct?
A: Correct. If the patient is unstable which is defined as “showing signs of poor perfusion.”
marshall williams says
thank u for explantions
vtxblue says
If there is no conduction thru the ventricles, thus no QRS, I’m confused why QRS complex appears on the strip…
Jeff with admin. says
In the rhythm strip where you just see p-waves, there is no electrical conduction through the ventricles. If you see a QRS that means that there is conduction for electricity through the ventricles.
Kind regards,
Jeff
NurseKary says
what is the difference between transcutaneous pacing and transvenous pacing? Is transvenous pacing with pacer wires like a post openheart patient? Thank you.
Jeff with admin. says
Transvenous pacing is achieved by threading a pacing electrode through a vein into the right atrium, right ventricle, or both.
Transcutaneous pacing is accomplished by delivering pulses of electric current through the patient’s chest from electrode pads, which stimulates the heart to contract.
Kind regards,
Jeff
taylor05 says
Hi , My ACLS expires in March and this is the best site ever thanks.
mary says
after so many, many years of acls… this finally makes sense.. your site is one i return to every time i retake acls!!!!!
thanks for making it make sense so i can do the right thing when it really counts!
Beverly says
I agree…I remember the megacodes in the ’70s…had been traumatized ever since with a lingering mental block: now resolved!
Thanks for the virtual anxiolytics 🙂
savvygirl says
Beverly
“Virtual anxiolytics” I LOVE IT!!!!!
Stacie
grace says
very excellent..its really good,. ill be having my acls training tomorrow,.and its nice for me,. i’m already advanced and understood it..thanks and i found this site..=)
Thomas S.Lis, MPH, PA-C says
Hi Jeff,
Great site. You have a concise and easy explanation for a subject that can be difficult and anxiety provoking. You incorporated the use of computer graphics very professionally. Thank you very much.
curlysue says
I am glad that I found this site. It is excellent and I also learn a lot from the answers given to comments or questions made by others. This is truly a rich experience. Thanks a lot!
stuckinmiddle says
My 2011 ACLS provider manual says to give Atropine before pacing?
Jeff with admin. says
You can give atropine while awaiting the TCP. However, you would want to give it after determining that the patient is not having an MI. 2nd degree HB Type II is often caused by MI. In the case of MI, the use of atropine can worsen the ischemia of the heart. TCP would be more appropriate that atropine if the patient has any ischemia of the heart.
Kind regards, Jeff
charlene malone says
This is the best study aide I have found for ACLS rhythm interpretation. As an OR nurse I take ACLS every other year and since I have never had to use it, always need to review. This is great!
patt thorn says
i have been diagnosed with this disease……what is my next course of action and can it cause death/
Jeff with admin. says
Hi Patt,
This site is not designed to diagnose or treat disease. You should do exactly what your physician tells you to do regarding any disease.
Kind regards,
Jeff
jennifer charles says
thank you jeff for the refresher
rnfomenko2012 says
It awesome
C L Soh says
Would you pace Second Degree Heart Block- Type 2 immediately although patient is stable and asymptomatic ? Or just standby and monitor first ? If no pacer available can IV Dopamine or Epinephrine be used instead ?
Jeff with admin. says
Hi CL,
If the patient is not symptomatic and is stable, you would standby and monitor. I would also seek expert consultation. I would do ACS (acute coronary syndrome) workup as 2nd degree heart block Type-2 is often associated with MI. –Kind regards, Jeff
Mylee Belle says
jeff, thanks for this info..
the other day, our team responded to a patient who presented in ED with an ACUTE MI…the very acute phase was overwhelming, we did rTPA as soon as it was available within the “golden hour”, and proceeded with the ACS work up…however, is it then logical and safe to assume that once we recognize 2nd degree heart block, we can start with ACS work up?(since the former is likely caused by MI) while preparing for more advance treatment such as pacing…?
Jeff with admin. says
Yes, it is logical and safe and actually the standard of care to work up a new onset heart block for suspected MI. You should immediately obtain an ECG and cardiac enzymes. The ACS protocol should be used until MI has been ruled out.
Kind regards,,
Jeff
jodi says
watching these rhythms along with differiated explination is very helpful study guide. Thank you
s.doough says
Thank you so much for this informative web site. This really helped reinforced the various rhythms-our nsg. floors now have tele beds and this site has been great-especially for recertification review.