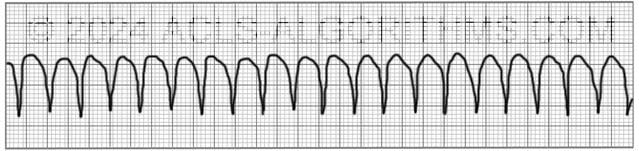
The pulseless ventricular tachycardia rhythm is primarily identified by several criteria. First, the rate is usually greater than 180 beats per minute, and the rhythm generally has a very wide QRS complex.
Second, the patient will be pulseless. And third, the rhythm originates in the ventricles. This is in contrast to other types of tachycardias which have origination above the ventricular tissue (in the atria).
Not all ventricular tachycardias are pulseless, and therefore, pulselessness must be established prior to beginning an algorithm. This is accomplished simply by checking a carotid or femoral pulse.
Pulselessness with a tachyarrhythmia occurs because the ventricles are not effectively moving blood out of the heart and there is, therefore, no cardiac output. Many tachyarrhythmias of a rate >150 will deteriorate into pulselessness if timely treatment is not given.
Pulseless ventricular tachycardia is treated using the left branch of the cardiac arrest algorithm. Click below to view the cardiac arrest algorithm diagram. When finished click again to close the diagram.
Cardiac Arrest Diagram

Click to view, and click again to close the diagram.
PALS Cardiac Arrest Diagram

Play the video below to see what a Pulseless Ventricular Tachycardia will generally look like on a defibrillator monitor. Allow several seconds for video to load. (4.03 mb)
Click for next Rhythm Review: Ventricular Fibrillation
Top Questions Asked on This Page
-
Q: What happens after the 2nd dose of Amiodarone is given and the patient is still in the same rhythm? Do we give a 3rd dose immediately or rhythm usually changes after 2nd dose?
A: A 3rd and even a 4th dose of 150 mg amiodarone may be administered. The only thing that needs to be taken into consideration is the 2.2-gram maximum dosage for 24 hours. Also, it is unlikely that the rhythm will remain VF or pVT long enough for you to get to the 3rd or 4th dose.
-
Q: What does refractory VT or VF mean?
A: Refractory pVT or VF means that the VF or pVT does not convert to a perfusing rhythm and continues to persist in spite of multiple attempts at conversion with defibrilation, acls drugs, and high quality CPR.
-
Q: After initiating CPR and assessing the rhythm, the patient is in VF/ pVT and the first shock is given, and CPR for 2 mins. Then rhythm check and in VT, should the pulse be checked to confirm pVT?
A: If there is no rhythm change and the same waveform of VT continues, you would not need to perform a pulse check. Performing the pulse check would delay the continuation of chest compressions. Once VT is pulseless it is very unlikely that any VT will be able to produce life-sustaining cardiac contractions.
Joan Williams says
Awesome Site.LOVE IT
Anonymous says
Hi good morning everyone
What is the step to follow in a patient who is awake, conversant with unstable BP (palpatory 50)
Is it possible that a pulseless patient awake and conversant?
TIA
Anonymous says
Sorry the reading in the cardiac monitor is ventricular tachycardia at 180bpm
Jeff with admin. says
First question: if you have a patient who is awake, conversant and has an unstable blood pressure you would want to determine the cause for the unstable blood pressure and treat it. If the cause is related to a tachyarrhythmia that is causing the patient to be unstable then synchronized cardioversion would be the appropriate treatment.
Second question:
If the patient is truly pulseless then they will not be awake and conversing with you. They have a pulse. You just can’t feel it.
In the situation, the patient probably just has poor blood perfusion and would need to be treated for that with the appropriate treatment.
Kind regards,
Jeff
Harley says
I think that being pulseless would mean no cardiac output therefore patient would not be perfusing and would not be Conscious
Lyn says
Hello! What if the first rhythm was asystole/PEA and you were able to give the first dose of epi and then after rhythm check, it becomes a shockable rhythm so we shift to the left branch of the algortihm, do you still give epi after 3 mins starting from the first administration (when it was administered for a nonshockable rhythm) or will the administration and counting of 3 mins be restarted after the 2nd shock? In other words, is the cycle of epi administration restarted when you shift from a nonshockable to a shockable rhythm?
Thank you very much!
Jeff with admin. says
Within the left branch of the cardiac arrest algorithm, epinephrine is always given during chest compressions. You’re the first dose is given, epinephrine is basically on its own timeline and is given every 3 to 5 minutes so you would be fine continuing with the same timeline from the PEA/asystole right branch.
Kind regards,
Jeff
Liz says
How can you tell the difference on ECG between PEA & pulseless v. tach? I know PEA is when a patient has a rhythm on ECG but has no pulse. Pulseless V. tach also has a rhythm but no pulse.
Thanks!
Jeff with admin. says
Any type of ventricular tachycardia that does not have a pulse will be considered pulseless ventricular tachycardia. It will never be considered PEA.
Even though pulseless ventricular tachycardia is technically Hey form of pulseless electrical activity, for the purposes of advanced cardiac life support, it is not because it is treated with the left branch of the cardiac arrest algorithm rather than the right branch of the cardiac arrest algorithm.
This is because pulseless ventricular tachycardia responds very well to high energy unsynchronized shocks.
Kind regards,
Jeff
Yolanda Wiid says
Why do we flush amiodorone with saline and not dextrose?
Jeff with admin. says
Normal Saline is fine. The reason why it is OK is because the bolus of amiodarone will be pushed in by the normal saline, and there will be an insignificant amount of mixing. Definitely not enough time or amount to cause any type of precipitation.
Kind regards,
Jeff
Hilgendh says
Hi, Jeff! Thank you so much for this site! Reading your answers to everyone’s questions is so helpful as well!
Sorry if i missed someone already asking this, but regarding monomorphic V-tach:
ACLS says if the patient is pulseless, give an unsynchronized shock of 120-200J, if they are unstable with a pulse give synchronized shock of 100J. My question is, if a v-tach rhythm is synchronizable, even if there is no pulse, why would we not synchronize? Does the extra 20 jouls make that much of a difference? Is there a physiological reason for this? Or is it just to make the algorithm easier?
Thank you!!!
Jeff with admin. says
First, thanks for your encouraging words!
Pulseless monomorphic VT responds quite well to unsynchronized defibrillation. In all likelihood, it would respond well to synchronize cardioversion as with VT with a pulse.
There is not a physiological reason for this, but since it is treated different than PEA and responds well to defibrillation it is included in the left branch of the cardiac arrest algorithm. It does simplify things.
Kind regards,
Jeff
Rhonda Gaines says
What a nice break to stop, read these comments and questions, it’s like even more review but personal. Thanks Jeff for providing a better way to learn and study. Far cry from the days of 2 long painful days of anxiety and tears….looking forward to PALS now
Edward says
Hello sir,
In your answer above (Q. 6) you mentioned to give Epi every 3-5 min regardless of anything else, and immediately after giving shock, so what if Amiodarone and Epi coincide together can I give them back to back or wait on Amiodarone till next CPR Cycle
Thank you
Jeff with admin. says
Yes, you can give amio and epi back to back during the same round of CPR if it is time for both of them to be given. Give epi then flush with 20 ml NS, then give amio and flush with 20 ml NS.
Kind regards,
Jeff
Raymond Navarro says
Good day! I just wanted to ask in the cardiac arrest algorithm during cor and lifepack advise no shock and continued 4 mins of cpr what do you mean about treat reversible causes sir?
Jeff with admin. says
Treating reversible causes means that you would attempt to identify any causes of the cardiac arrest that may be reversed. You would want to quickly review the H’s and T’s of ACLS to see if you can identify any possible reversible causes. Here is a review that you can look over which will explain the most common reversible causes that might be discovered.
H’s and T’s of ACLS
Kind regards,
Jeff
Raymond Navarro says
Hello sir gud day I just want to ask after 2 mins of cpr and lifepack advices no shock, and continued 4 mins of cpr. In the cardiac arrest algorithm,what you mean to treat reversible causes?
Jeff with admin. says
In the case that the cardiac arrest is being caused by something that is reversible like opioid overdose or foreign body airway obstruction you would want to identify this and treat it.
Kind regards,
Jeff
khaled says
it is known as five Hs and five Ts
Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hyper-/hypokalemia, Hypoglycemia, Hypothermia
________
Toxins, Tamponade(cardiac),Tension pneumothorax, Thrombosis (coronary and pulmonary), and Trauma
Mrs Nakajima says
Hello,
General question here. What is the difference between the ‘red’ shock icon and the ‘yellow’ shock icon? Is it voltage difference?
Great site. Need to cram all this information in my head again in a month, but need certification to access more ‘opportunity’ to become familiar with using the knowledge, so am understanding why acquisition of this body of knowledge is a routine and periodic yearly requirement!
Thanks!
Jeff with admin. says
The first yellow shock icon is representative of the initial shock. The red shock icon is representative of all shocks that come after the initial shock.
Please let me know if you have any other questions.
Kind regards,
Jeff
Marcie says
i have been away from acute care/critical care nursing for 8 years and now i am going back and needs ACLS certification. Are you posting the latest or current practice or changes now in practice? i don’t have a book but have registered on February 17 Flexd Med.
Jeff with admin. says
Everything on the website is current with the latest American heart Association guidelines. The entire website is designed to be used as a standalone resource or in conjunction with the American Heart Association provider manual’s. I do have many students that use the site without the provider manual and do great.
Kind regards, Jeff
francis s says
I have been using your site since 5 years for my ACLS ,I found that it was so helpful and yesterday I did my ACLS . I referred this site to my friends too
Thanks Jeff
Great site
Wendy Gaus says
Just clarifying….What do you mean by IVP? I suspect you mean IV Push and not IVPB or intravenous pyelogram (IVP) which is what it traditionally stands for. Thanks, Wendy
Jeff with admin. says
Yes, in this case, IVP stands for IV Push.
Kind regards,
Jeff
Laura Vandewaal says
This is the most interesting conversation I have run into and make refreshing of the coarse so easy l love it
Thanks