
The most common cardiac arrhythmia, atrial fibrillation, occurs when the normal electrical impulses that are generated by the SA node are overwhelmed by disorganized electrical impulses in the atria.
These disorganized impulses cause the muscles of the upper chambers of the heart to quiver (fibrillate) and this leads to the conduction of irregular impulses to the ventricles.
For ACLS, atrial fibrillation becomes a problem when the fibrillation produces a rapid heart rate which reduces cardiac output and causes symptoms or an unstable condition.
When atrial fibrillation occurs with a (RVR) rapid ventricular rate (rate > 100 beats/min), this is called a tachyarrhythmia. This tachyarrhythmia may or may not produce symptoms. Significant symptoms that occur are due to a reduction in cardiac output.

The following is a list of the most common symptoms.
- palpitations or chest discomfort
- shortness of air and possibly respiratory distress
- hypotension, light-headedness and possibly loss of consciousness
- peripheral edema, jugular vein distention, and possibly pulmonary edema
For the purpose of ACLS, it is important to be able to recognize atrial fibrillation when the patient is symptomatic. On an ECG monitor, there are two major characteristics that will help you identify atrial fibrillation.
- No p-waves before the QRS on the ECG. This is because there are no coordinated atrial contractions.
- The heart rate will be irregular. Irregular impulses that the ventricles are receiving cause the irregular heart rate.
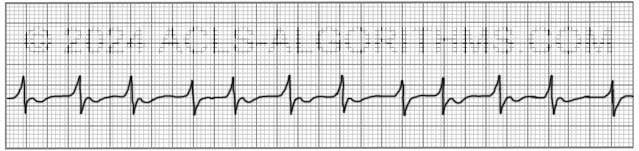
When the heart rate is extremely rapid, it may be difficult to determine if the rate is irregular, and the absence of p-waves will be the best indicator of atrial fibrillation.
ACLS Treatments:
For the purposes of ACLS atrial fibrillation is treated when the arrhythmia/tachyarrhythmia produces hemodynamic instability and serious signs and symptoms.
For the patient with unstable tachycardia due to a tachyarrhythmia, immediate cardioversion is recommended. Drugs are not used to manage unstable tachycardia. The appropriate voltage for cardioverting unstable atrial fibrillation is 120-200 J.
Cardioversion of stable atrial fibrillation should be performed with caution if the arrhythmia is more than 48 hours old and no anticoagulant therapy has been initiated due to the risk of emboli that can cause MI and stroke.
Below is a short video which will help you quickly identify atrial fibrillation on a monitor.
Please allow several seconds for the video to load. (5.11 mb)
Click for next Rhythm Review: Other Tachycardias
Top Questions Asked On This Page
-
Q: To treat a patient with rapid atrial fibrillation (HR >180bpm), can calcium channel blockers be given to help control the rate?
A: Yes, in some cases, calcium channel blockers are a good choice to help control atrial fibrillation with a rapid ventricular rate.
-
Q: What are atrial fibrillation and atrial flutter considered in terms of narrow or wide QRS complexes?
A: Unless there is an underlying block the QRS complex will typically be normal/narrow. There is the possibility of occasional wide QRS complexes due to abnormal ventricular depolarization via an accessory pathway.
-
Q: What does the DC before the word cardioversion stand for?
A: DC cardioversion simply means direct current cardioversion.
Joyce says
The difference between a flutter and a fib when looking at a EKG strip is that a flutter have p waves and a fibs don’t have p waves? I have trouble reading and differencing the two rhythm on a strip. Thank you.
Jeff with admin. says
Atrial FIBRILLATION, you will not see any p-waves. You may some a wavy line, but you should not see anything that resembles a consistent wave.
Atrial FLUTTER, you will see some characteristic flutter waves at a regular rate of 240 to 440 beats per minute. Individual flutter waves may be symmetrical, resembling p-waves, or may be asymmetrical with a “sawtooth” shape, rising gradually and falling abruptly or vice versa.
Kind regards,
Jeff
Christine says
I’m a medic student just beginning my cardiology section… I see an algorithm for Sinus Tach and Sinus Brady, but do you have an algorithm for A-Fib and A-Flutter as well?
Jeff with admin. says
On the site I do try and stick with ACLS as taught through the AHA ACLS provider manual.
Atrial Fibrillation and Atrial Flutter are handled within ACLS when they are symptomatic which is usually due to a rapid ventricular rate. For the purposes of ACLS, these rhythms are handled using the tachycardia algorithm. The treatment for stable atrial fibrillation and atrial flutter is beyond the scope of the site and also beyond the scope of ACLS.
Kind regards,
Jeff
johnYPQ says
After reading all this i am getting if you come accross a patient in non controlled A-Fib for more than 48 hrs
if the patient is stable get them to a medical facility
if they are considered unstable and you must intervene before EMS arrives, then take the chance, cardiovert 100 J, then ?????
Jeff with admin. says
If EMS has not arrived, there will be no way to perform cardioversion. An AED is not capable of performing cardioversion. The AED will say no shock advised if it does not see VT or VF.
If EMS is present in a scenario with unstable A-fib it would be advised to communicate with the dispatch for instructions on treatment. There is a high likelihood of causing a stroke if the patient has had uncontrolled atrial fibrillation for longer than 48 hours.
Most likely, folks with a-fib are going to have symptoms that will take them to the hospital before they are unstable.
In summary, your best option is to seek expert advice through dispatch before intervention.
Kind regards, Jeff
Punky104 says
I am new to ACLS. A-FIB with RVR looked alot like the monitor strip of SVT where the P waves were buried in the QRS.And with the heart rate being so fast in both cases, unless the irregular rate of A-FIB is blatantly irregular, is there another way to differentiate between the two when looking at a monitor?
Jeff with admin. says
You will usually be able to recognize the irregular rate seen with A-fib + RVR and this is the easiest way to differentiate the two. After you see several of them, it gets a bit easier. However, there are times (very rapid rate) when you may not be able to tell the difference. Technically, SVT and Atrial Fibrillation with RVR are both Supra-ventricular arrhythmias and can be treated as such. Giving adenosine for either one would slow the heart rate down and allow you to see what is going on (p-waves or no p-waves).
Kind regards,
Jeff
cooten says
so you cardiovert a-flutter at 50 – 100 J and a-fib is cardioverted at 120 – 200 j, but when stable and tachy they can both be treated with cardizam?
Jeff with admin. says
If the a-fib or a-flutter is causing a rapid ventricular rate then, yes, giving cardizem and also getting a cardiology consult would be a good choice in most cases.
Kind regards,
Jeff
Danny Lambert says
Jeff, I’m wondering what to due with AF and a vent. rate of, say, 150 creating an unstable patient AND the patients rhythm present for 3-4 days w/o anti-coagulation.
Your suggestions.
Thanks!!
Danny
Jeff with admin. says
I would suggest performing an STAT TEE (trans-esophageal echocardiogram) to rule out thrombus. Once thrombus is ruled out, I would cardiovert.
You could also start a infusion of a calcium channel blocker (Cardizem) which would hopefully have a slowing effect on the heart. It would also be appropriate to start some type of anti-coagulant (Heparin Sodium).
kim tane says
but is it ok to cardiovert a person that is over 48hr (say 3days) if the person is already on warfarin?
and when you use the term ‘cardioverson’, does that actually mean ‘syncronised cardioverson’ or a ‘synchronised shock’?
Jeff with admin. says
Kim, You would need to do a TEE to rule out the presence of left atrial
thrombi before cardioversion even after 3 days. Cardioversion can be either synchronized or unsynchronized. To say synchronized cardioversion would be equal to saying synchronized shock. The best way to describe the action would be synchronized cardioversion. When someone says “shock” it usually means unsynchronized cardioversion.
Deborah says
What is the difference between synchronized or unsynchronized cardioversion?
Thanks!
Jeff with admin. says
You will find your answer here.
https://acls-algorithms.com/synchronized-and-unsynchronized-cardioversion
Kind regards,
Jeff
http://www.acls-algorithms.com
PAULA BLANCHARD says
What is the 48 hour rule for cardioversion of unstable atrial fib or flutter?
Jeff with admin. says
For unstable afib or flutter, you would need to take this into consideration:
“Two strategies have evolved to prevent
stroke after cardioversion. In patients with
atrial fibrillation for longer than 48 hours, the
conventional approach is to give anticoagulants
for at least 3 weeks before and for 4 weeks
after cardioversion.3–5 A newer approach, used
for the past 10 years, is to use transesophageal
echocardiography (TEE) to guide the decision
about when to perform cardioversion: TEE is
used to rule out the presence of left atrial
thrombi before cardioversion, thus permitting
cardioversion sooner and with a shorter period
of anticoagulation before cardioversion.”
Quoted from: http://ccjm.org/content/69/9/713.full.pdf
Ninh Le says
Thank you, Jeff! The website is awesome!!!!!!!!!!
Patricia Nolan says
Then what is the treatment for this?
Jeff with admin. says
If the patient unstable, cardioversion. If stable there are a variety of treatments. (anitcoagulation, cardioversion, medications for rate control, etc.) —–Jeff
Robin Harvey says
Is there a way to make the screen larger? The a-fib example is too fine for me to see. 🙂
Jeff with admin. says
You can enlarge the screen but clicking on the expand icon in the lower right hand corner of the video viewer for each video. This will take the screen to the largest size.
With regard to A-fib. You may not be able to see the fibrillation and this is true in real time on a monitor. A-fib. Is recognizable because of the irregular rate and lack of p-waves. More often an a-flutter rhythm will be visible. I hope this makes sense.
Kind regards,
Jeff
kathleen gregory says
Is it possible to go “in and out” of a-fib thereby forming atrial clots? Then along comes someone that decides to cardiovert without an echo, etc. I guess if they’re circling the drain you have to cardiovert. Agree with s.levine though
Jeff with admin. says
When the onset is a longer period of time, blood clots can form in the circulatory system due to the pooling of blood in the atria of the heart. Cardioversion should only occur if the patient is unstable and it is not possible to perform an echo. Otherwise, consult an expert and get an echo. Jeff
Ann Barrow says
Do you ot have standard algorithm pages with steps shown find them easier to follow then narratives
zaaba PRABA says
very useful question and answers for the general practitioners and primary care physicians
zaaba PRABA says
Is Vernakalant a useful drug for rapid conversion of Afib any side effects?
Jeff with admin. says
During clinical evaluation, 6 deaths occurred in the vernakalant groups versus none in the other groups (placebo or amiodarone). Prescrire Int. 2012 May;21(127):119-22.
I don’t think that I would consider this a safe alternative.
Kind regards,
Jeff
Jeff with admin. says
Hi Tinisans,
The comment from S. Levine meant that the atrial fibrillation was onset of greater than 48 hours.
When the onset is a longer period of time, blood clots can form in the circulatory system due to the pooling of blood in the atria of the heart.
Hope this helps you understanding
Kind Regards,
Jeff
acls-algorithms.com
s. levine says
Be very careful about cardioverting afib more than 48 hours old without anticoagulant therapy for fear of creating emboli that cause MI or stroke