
Second degree heart block which is also called Mobitz 1 or Wenckebach is a disease of the electrical conduction system of the heart in which the has progressive prolongation until finally the atrial impulse is completely blocked and does not produce a QRS electrical impulse.
Once the p-wave is blocked and no QRS is generated, the cycle begins again with the prolongation of the PR interval.
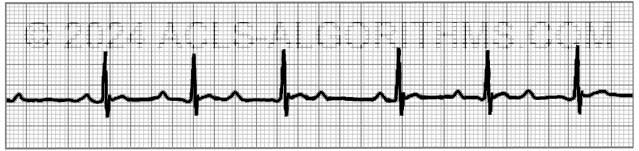
One of the main identifying characteristics of second-degree AV block (Type 1) is that the atrial rhythm will be regular.

In the above image, notice that the p-waves are regular, the PR-interval progressively gets longer until a QRS is dropped and only the p-wave is present.
PR Interval
The PR interval is the electrical firing of the atria and conduction of that electrical impulse through the AV node to the ventricles.
Although second-degree AV block (Type 1) is not typically clinically significant for ACLS, recognition of the major AV blocks is important because treatment decisions are based on the type of block present.
Second-degree AV block (Type I) may be a normal variant in the conduction system of the heart and is usually due to a reversible conduction block at the level of the AV node. There are several disorders that can cause Second-degree AV block (Type I). The most common causes are listed below:
Causes of Second-degree AV block (Type I):
- Increased vagal tone (well trained athlete)
- Medications that inhibit AV node conduction (amiodarone, beta-blockers, calcium channel blockers, digoxin)
- Myocarditis caused by infections
- Hypoxemia (see more in infants and children)
- Cardiac surgery
- Myocardial infarction
- Any condition that stimulates vagal tone
Below is a short video which will help you quickly identify second-degree AV block (Type 1) on a monitor. Please allow several seconds for the video to load. (3.69 mb)
Click for Next Rhythm Review:
Second Degree AV Block (Type II)
Top Questions Asked On This Page
-
Q: In second degree AV block what is the meaning of “QRS dropped?” Does it mean less than 3 square?
A: It means that the QRS is not present. You will most likely see a p-wave but no QRS. The impulse that is produced in the SA node (p-wave) is not transferred through the AV node, and therefore no QRS wave is seen on the monitor.
-
Q: With 2nd-degree Type I, is atropine warranted or should we go straight to pacing?
A: Atropine should come before the application of pacing as long as the administration of atropine will not delay the use of pacing in an unstable patient.
-
Q: Why would the ventricle not fire a beat following the AV node non-conductive beat/ p wave non-conductive beat?
A: 2nd Degree Block Type 1 (Mobitz I) is usually due to a reversible conduction block at the level of the AV node. Some of the reversible causes are caused by medications such as beta-blockers, calcium channel blockers, and digoxin. Other reasons are inferior MI, myocarditis, increased vagal tone, and post heart surgery.
The AV node cells are malfunctioning, and they tend to fatigue progressively until they fail to conduct an impulse.
Forever Grateful says
Awesome training. Walked into my initial ACLS course like a boss! ~Thx a mill!!!
ginger says
These are a big help! Thanks
JULIO SANTIAGO says
video suggested junctional signal QRS after the dropped QRS,
should there be no QRS? Then a normal PQRS
Jeff with admin. says
That’s right. After the dropped QRS complex, there would be a normal PQRS. Kind Regards, Jeff
rathmagg says
I’m not sure what is meant by “The main identifying characteristic is that the atrial rhythm is regular.” I see that the ventricular rhythm is reg except for the dropped QRS. The p waves are reg, but the distance between p waves clearly is not. Am I missing something?
Thanks for all the work you’ve put into this.
Maggi
Jeff with admin. says
Atrial rhythm = atrial contraction = p-waves.
The p-waves are regularly spaced. (5 large squares between each p-wave).
2nd degree block type 1’s primary characteristics are the atrial rhythm (p-waves) is regular with equidistantly spaced P-waves and a progressively longer PR interval. At the end of the progressively longer PR interval series, you will see a dropped QRS complex and then the process starts over.
I hope that helps.
Kind regards, Jeff
rathmagg says
Thanks for changing the strip. Much clearer now. 🙂
Jeannine Porod says
Thanks. Just diagnosed with this a d explained it to me
elainepractitioner@gmail.com says
A poem I recall, to help us remember:
“Long, longer, longer- Drop-
Mobitz 1 or Wenckebach!”
leederpack says
Will use that – thx
Joe Momma says
I could do without the suspenseful background music in the videos.
SonyaPoole says
I thought the music was fitting haha. Video definitely helps a lot!
Nayner2216 says
I too like the music. Lol
Leigh says
I love the music!!! Very fitting.
jkerns56 says
I had to turn my sound off it was so distracting.
Nancyortlip says
Intense music for an intense situation. Real life doesn’t allow us to simply tune out the distractions. I think it’s perfect.
Kenneth Bradshaw says
In a learning situation where students are first learning the rhytms, this music is most certainly very distracting. If music or the tv were loudly blaring in the patients room during a code blue, the physician would direct that it be turned off or down, as it too would be distracting…
jgschoeneck says
Turn off the sound, ha ha
aba says
Hi Jeff,
I’m new to this. can you please explain the difference between Mobitz I and II. All I see is dropped QRS in both!
Jeff with admin. says
With Mobitz I, the PR interval will get longer and longer and then there will be a p-wave with no QRS.
Mobitz II, the PR interval will be the same, but there will be p-waves without any QRS complexes.
That is the easiest way to tell the difference. Look at this page and the page below a couple of times and make sure to watch the videos at the bottom of each page. It will get easier as you learn to recognize the PR interval.
2nd Degree Block Type 2
Kind regards,
Jeff
Blonde4fun says
While I know the definition of Type 2 HB and 3 Degree HB, it is still difficult for me to actually recognize (especially if the monitor is moving the rhythm strip across the screen). Any suggestions of quick recognition would be appreciated. Love your site. So helpful!
Jeff with admin. says
These can be tricky blocks to recognize. Here is what will do the trick. For a month do this: Each day you work, look at 2 different examples of each rhythm that you want to be able to recognize. Go through the entire interpretation process for each rhythm. You might have to spend 5 or 10 minutes per day. After a month you should be able to quickly recognize each. In this case, practice does really make perfect.
Kind regards,
Jeff
Erika says
I always remembered this way:
“P’s short-longer-longer-drop then you have a Wenkebach” (and its a PATTERN that repeats)
“If some P’s dont get through, then you have a Mobitz II”
“If P’s & Q’s dont agree, then you have a 3rd degree” (CHB)
Jeff with admin. says
Thanks for sharing. Good stuff! Kind regards, Jeff
bisabelh says
Why isnt type1 significant for ACLS but type 2 is? I understand that the dropped QRS could lead to complete block, but if type 1 is also missing the complex…
Thnx!
Jeff with admin. says
Type 1 Mobitz I is typically caused by a reversible conduction block at the level of the AV node.
Malfunctioning AV node cells tend to progressively fatigue until they fail to conduct an impulse. The AV node cells then recover and the process typically begins again.
While Mobitz I is typically caused by a functional suppression of AV conduction with reversible causes (i.e. drugs, reversible ischemia), Mobitz II (Type II) is more likely to be due to structural damage to the conducting system (i.e. infarction, fibrosis, necrosis) which is more likely to degrade to complete failure in conduction and the resulting Third Degree Block (complete block).
Hope that helps.
Kind regards,
Jeff
Angie says
Would you be able to place a red arrow over where the dropped QRS would be?
Jeff with admin. says
Thanks for the suggestion. That is a great idea. It’s done.
Kind regards,
Jeff
Susan says
Again, just what I needed after 20 years of being away from the monitors. Thank you so much for this all.
gerry says
thanks for the link on Heart Blocks. I am just beginning my review of the material for ACLS and am reviewing general information first to be able to put the specifics of ACLS in context. This brief link is worth a look
p.k.julie@gmail.com says
Great info. Great for ACLS and just for overall cardiac knowledge. In regards to blocks, hat is a Bundle Branch Block then? Does it fall in one of these types of categories that you have mentioned?
Jeff with admin. says
Bundle branch blocks are blocks that occur in the distal conductive system of the heart where as all of the blocks discussed within ACLS are nodal blocks that occur at the SA or AV node. This article may help clarify: Heart Blocks
James says
In Mobitz I will the p waves always march out to be regular?
Jeff with admin. says
Yes, The P waves will always march out regular.
Kind regards,
Jeff