Ventricular fibrillation (VF) occurs when there are uncoordinated contractions within the ventricles of the heart. The primary cause of VF is hypoxia (lack of oxygen) to the heart muscle, which causes hyperirritability in the cardiac muscle tissue.
As a result, multiple muscle cells within the ventricles simultaneously fire as pacemakers causing a quivering or fibrillation that is ineffective for adequate cardiac output.
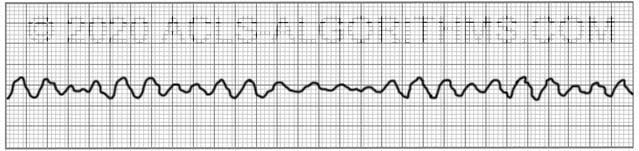
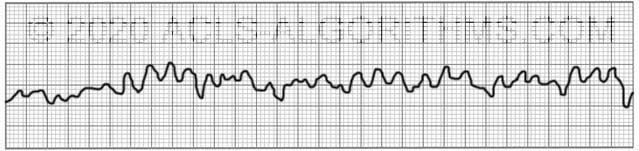
The two images show what ventricular fibrillation will look like on an EKG rhythm strip.
VF can rapidly lead to heart muscle ischemia, and there is a high likelihood that it will deteriorate into asystole.
Ventricular fibrillation is treated using the left branch of the cardiac arrest algorithm. Click below to view the cardiac arrest algorithm diagram. When done click again to close the diagram.
Cardiac Arrest Diagram

Click to view, and click again to close the diagram.
PALS Cardiac Arrest Diagram

Ventricular fibrillation is always pulseless and must be confirmed by EKG or defibrillator monitor. Defibrillation is the treatment of choice and should occur as soon as possible.
The video below shows an example of what ventricular fibrillation will look like when you see it on the defibrillator monitor. Please allow several seconds for the video to load. (7.24mb)
Click for next Rhythm Review: Pulseless Electrical Activity
Top Questions Asked on This Page
-
Q: Why does it say VFib is always pulseless? My thinking is an organized rhythm with no pulse will be PEA, then should be treated as on R branch of the cardiac arrest algorithm.
A: Ventricular fibrillation is not an organized rhythm. It is a chaotic and disorganized rhythm. There is no organization to the rhythm. There are no p-waves and no QRS complexes.
-
Q: Which concentration of Lidocaine is given intravenously in ACLS considering that there is the local anesthetic as well. Is the 2% safe?
A: Typically, lidocaine for IV infusion is mixed 2000 mg lidocaine in 500 ml. This works out to a 4 mg/ml dilution.
Two percent lidocaine is a 20 mg/ml. This 20 mg/ml would need to be diluted to obtain the 4 mg/ml dilution.
You would not want to give 2% lidocaine without diluting to 4 mg/ml. -
Q: When does the sodium bicarb injection need to be administered and when does the lidocaine IV need to be administered?
A: Here is the AHA position on Sodium Bicarbonate:
“In some special resuscitation situations, such as preexisting metabolic acidosis, hyperkalemia, or tricyclic antidepressant overdose, bicarbonate can be beneficial (see Part 10: Special Circumstances of Resuscitation).
However, routine use of sodium bicarbonate is not recommended for patients in cardiac arrest.”
Here is the AHA position for Lidocaine:
“There is inadequate evidence to support the routine use of lidocaine after cardiac arrest. However, the initiation or continuation of lidocaine may be considered immediately after ROSC from cardiac arrest due to VF/pVT.
Lidocaine may be considered as an alternative to amiodarone for VF/pVT that is unresponsive to CPR, defibrillation, and vasopressor therapy.
Mlandeli J Ncube says
This was helpful indeed!!!
CARIMA SOLAIMAN says
I would like to ask, during a code in the 2nd cycle still it is vfib, , can you please explain when will i give epi, and amiodarone? Is it allowed to give both after the other?
ACLS says
For ventricular fibrillation, Epinephrine will be given after the second shock during CPR. Amiodarone or lidocaine may be given after the third shock during CPR.
Kind regards,
Jeff
doves78353@yahoo.com says
What exactly is a witnessed and unwitnessed cardiac arrest?
ACLS says
Witnessed cardiac arrest means that someone witnessed a person experiencing the cardiac arrest prior to and after the collapse of the person.
Unwitnessed cardiac arrest means that no one was present when a patient collapsed and cardiac arrest took place.
Kind regards,
Jeff
SUDHIR DEY says
HeI : If I want to give Lidocaine in absence of Amiodarone, I will take 0.2 ml lidocaine containing 20 mg/ml. so it will be 4 mg in 0.2 ml . Then take 0.8 mi normal saline more. It will be 4 mg/ml which is then ready to infuse. Is it correct? otherwise pl tell your suggestions how to make ? Thanks.
Jeff with admin. says
Typically, lidocaine for IV infusion is mixed 2000 mg lidocaine in 500 ml. This works out to a 4 mg/ml dilution.
Two percent lidocaine is a 20 mg/ml. This 20 mg/ml would need to be diluted to obtain the 4 mg/ml dilution.
You would not want to give 2% lidocaine without diluting to 4 mg/ml.
Dzina Rozava says
Kindly keep in mind that concentration depends on total volume. If you take 0.2ml of 20mg/ml solution, the concentration in those 0.2ml still will be 20mg/ml. You would rather want to add 4ml more of normal saline to 20mg/ml solution to dilute it further to 4mg/ml concentration. This way you will have 20mg of lido in 5 ml of normal saline, which gives you concentration of 4mg/ml.
Eula I says
Greetings Jeff: I am going thru the Vfib section in your tutorial, “Lidocaine may be considered as an alternative for VF/pVT that is unresponsive to CPR, defibrillation……etc”……..However; doing a bit more research on my own, i will quote from from a book on Hemodynamic monitoring by Gloria Oblouk Darvoric on Page 327:
“Lidocaine now appears in the ACLS algorithm for Stable Ventricular Tachycardia (as a second choice to amiodarone), which is associated with acute myocardial ischemia or injury. This drug no longer appears in the algorithm for ventricular fibrillation or unstable ventricular tachycardia, but its use would be acceptable in resuscitation attempt” …………………Please explain as I found it misleading or maybe my lack of understanding.
Thanks
Jeff with admin. says
It is true that lidocaine is not mentioned on the ACLS algorithm diagram for pulseless VT and VF. However, lidocaine is discussed in the AHA ACLS provider manual. It is discussed on multiple pages, but the main page that you can reference is page 100.
Here is a quote from that page. “If amiodarone is not available, providers may administer lidocaine.” This quote is found under the section labeled Shock and Antiarrhythmics. On this page, it also lays out the indications for lidocaine and the mechanism of action.
Kind regards,
Jeff
Ralph Burger says
– From an “End User”
Good Afternoon,
I am one of the 4% of survivors of a VFib event in 2014. I’m proud of my EMS team and doctors at UCSD Sulpizio Cardiovascular Center in La Jolla, CA.
My family thanks all who participated in my resuscitation and care. This is one very happy and blessed of the 2000 additional lives that might be saved each year in North America.
Please do all that you can. My team gave it their all. 9 epi’s, 11 shocks and amniodarone was my “30 minute E ticket” to a Vfib death to life again.
RFB
Anthony says
I have been reading multiple studies lately around the world regarding what appeared to be asystole on the monitors (checking different leads, checking different monitors) only to find out by ultrasound that the heart was actually in fine or very fine vf, too fine for the monitors to register. And that this is all the more likely in a witnessed arrest. Many comment that we may be missing a life saving opportunity. So I am curious if you agree that, since high quality CPR is the absolute most effective treatment for asystole, in the case of a witnessed cardiac arrest; rather than take valuable seconds away from high quality cpr to defibrillate what is technically asystole on the monitor; isn’t it true that we should be giving these patients every shot at life possible, and therefore try adding amiodarone which, if the patient is in the arrhythmia of very fine or fine vf; at least has the possibility of converting that fine or very fine vf into……ANYTHING, which is better than asystole or PEA– perhaps a course vf or a fine vf thats at least now able to be picked up on the monitor? NOW you can see the vf and justify the seconds taken away from high quality CPR to defibrillate? I look forward to your response
Jeff with admin. says
I agree with you completely. If there is a witnessed cardiac arrest and the initial rhythm is asystole, I would strongly suspect that the rhythm is not asystole but rather fine ventricular fibrillation. In this circumstance, especially if you knew that there were no existing comorbidities or disease processes, I would definitely agree that it would be prudent to attempt defibrillation.
Kind regards,
Jeff
anthony says
Jeff, thanks so much for your reply!
In my case, all of what you just is exactly accurate, including knowledge of the patient being absent of comorbidities or disease precesses. It was witnessed and it was literal sudden death, but because the “official rhythm” on the monitor was presenting as asystole, the EMS worker criticized my choice to not adhere strictly to the asystole algorithm and questioned why would someone use an arrhythmic on a heart that is in asystole, not an arrhythmia? A cardiologist (that I do not even know) backed me up and said, exactly like you, that especially being a witnessed cardiac arrest, the patient had a high probability of actually being in fine VF; and his response was that he agrees with my action and the clinical justification of why I suspected the possibility of fine VF unable to register on the monitors (as all these other studies show ultrasonic evidence of), and why I chose to give this patient every possibility I could at life by not ignoring this knowledge that recent studies show and address this highly possible arrhythmia instead of just strictly adhere to the asystole algorithm; and to choose to address this highly possible arrhythmia via treatment with amiodarone, which took zero seconds away from the continuance of highly effective CPR instead of risking taking the time to defibrillate away from uninterrupted CPR when “technically” (on the monitor) the rhythm was an unshockable asystole. He said that administering amiodarone, while not part of the asystole algorithm, was not only an appropriate intervention; but also an indicated one–citing that my reasoning is correct; that he agreed current science has shown that very fine VF, often extremely often unidentifiable on monitors, is common in witnessed cardiac arrests (as this was) and that based on that knowledge, the administration of amiodarone was a safe, appropriate and indicated intervention to take all possible measures to save a pulseless patient in a witnessed code. I know if it was my loved one, I would want the healthcare worker to take very possible shot at saving my loved one; and that would include addressing the high possibility of a true rhythm of fine VF and administering the AHA’s first choice antiarrythmic of amiodarone; hoping that will break the vf completely (ideally into SR or SB), or at least make the vf able to be registered on the monitor and then have the green light to switch to the left and add defibrillation. Do you agree?
Jeff with admin. says
I definitely think that defibrillation would be a pertinent option, but I’m not sure if I would resort to the use of amiodarone simply because there is no evidence to show that the use of amiodarone improves survival to hospital discharge. I suppose if the administration of amiodarone did not take away from CPR or early defibrillation then the administration of amiodarone would not be contra indicated. I suppose it could be a viable option and couldn’t heard a patient that is already going to be dead. Kind regards, Jeff
anthony says
Hey Jeff!
I know what you mean, I have read the studies that noted that in all cases amiodarone actually DID show an increase in survival to hospital discharge; but characterized the 2-4% (depending on the study) to be “not statistically significant”. But my point in giving the amiodarone was not to use amiodarone as an actual treatment modality as an isolated means to treat the “non sinus rhythm”; but rather just to exert its antiarrythmic effects on a heart that underwent witnessed sudden death (which we later found out to be due to a pulmonary thrombus) has a high likelihood of being in fine VF; and thereby just possibly break the very fine VF that cant be picked up by the monitors into anything that CAN be; be it just breaking it enough to make it more course and thus be able to now follow the VF algorithm because it now allows us to see that its in VF; or break the very fine VF into any other rhythm that can register on the monitor; and likewise we can now treat it by the appropriate algorithm. To have taken precious seconds away from high quality CPR in order to have everyone clear the patient and deliver the shocks, when the rhythm on the monitor is asystole, would have opened us up to legal malpractice issues for those precious seconds lost to high quality CPR without a guarantee that the heart was in VF. Whereas giving the only recommended first choice antiarrythmic (amiodarone) took absolutely not one second away from nonstop high quality CPR; and may have allowed the highly likely VF to register on the monitor and now allow us to follow the VF algorithm and legally be right to take those valuable seconds from CPR to give the shocks. By administering the amiodarone, it gave a harmless additional option to show proof on the monitor of the undeniably high possibility that this patient was in very fine VF, and thus allow us to focus on interventions that have the ability to improve survival such as high quality chest compressions and defibrillation. Do you now see why the cardiology expert that was consulted agreed with my decision to administer amiodarone “while not part of the asystole algorithm, was not only an appropriate intervention; but also an indicated one”? And, based on the science, do you agree?
(I also read a recent study that concluded that Amiodarone and lidocaine are associated with slightly better survival outcomes compared with placebo in patients with non-shockable-turned-shockable out-of-hospital cardiac arrest (OHCA), according to a randomized double-blind study published in Circulation. In all, 16 (4.1%) amiodarone, 11 (3.1%) lidocaine and 6 (1.9%) placebo-treated patients survived to hospital discharge (p=0.24). Over one-half of these survivors were functionally independent or required minimal assistance. Drug-related adverse effects were infrequent.
They wrote “Conclusions—Outcome from non-shockable-turned-shockable OHCA is poor, but not invariably fatal. Though not statistically significant, point estimates for survival were greater after amiodarone than lidocaine or placebo, without increased risk of adverse effects or disability, and consistent with previously observed favorable trends from treatment of initial shock-refractory VF/VT with these drugs. In addition, “improving absolute survival by merely 4% in this patient population means more than 2000 additional lives might be saved each year in North America from non-shockable-turned-shockable OHCA alone. So while some may argue that 4% may not be largely considered “statistically significant”, the families of the 2000 additional lives saved by the administration of amiodarone, without increased risk of adverse effects or disability from amiodarone, would argue it to be incredibly significant.”)
….But I would like to know if, in your expert opinion, agree with my administration of amiodarone; “while not part of the asystole algorithm, was not only an appropriate intervention; but also an indicated one” based on the science we now know about witnessed sudden deaths.
Thanks so much for your thoughts and expert opinion
Jeff with admin. says
I think you made a wise decision. I agree with your administration of amiodarone.
Kind regards,
Jeff
Fawad Ahmad azamy says
Dear all and seniors, as you know cardiac arrest is an emergency and the ACLS team should work their best and hard and also you know we have deferent choices like shockable and non shockable rhythm and also we have an option if defibrillator is available and rhythm is shockable so he should give him shock but if rhythm is shockable but we don’t have defibrillator so we have to continue the Effective CPR and epinephrine and amiodarone to save patients life, I am agree with effective CPR and others options like epinephrine and amiodarone too. And we should look for patients response at the time of ACLS algorithms. Thanks
Dr Fawad Ahmad Azamy
Emmanuel Maro says
This is the great site with simplified contents for preparations before acls certification.
It helped me to pass my acls training.
Great job.
Llamina Ralls says
The first dose of amioderone is given after the third schock. What is the time frequency for giving the second dose of amioderone (150 mg). Also do the antiarrythmics need to be given after a schlock?
Jeff with admin. says
Minimum is 3-5 minutes of high quality cpr after the first dose. Most important thing is that the first dose be adequately circulated before a second dose is given.
Kind regards,
Jeff
Thu Ng says
Please help w some confusions here: Why it says VFib always pulseless?. My thinking is :an organized rhythym w no pulse will be PEA, then should be treated as on R branch.
Thanks Jeff.
Jeff with admin. says
Ventricular fibrillation is not an organized rhythm. It is a chaotic and disorganized rhythm. There is no organization to the rhythm. No p-waves and No QRS complexes.
Kind regards,
Jeff
DOREEN says
Hello, thank you for the information. Which concentration of Lidocaine is given intravenously in ACLS considering that there is the local anaesthetic as well.Is the 2% safe?
Jeff with admin. says
Typically lidocaine for IV infusion is mixed 2000 mg lidocaine in 500 ml. This is a 4 mg/ml dilution.
2% lidocaine is a 20 mg/ml. This 20 mg/ml would need to be diluted to obtain the 4 mg/ml dilution.
You would not want to give 2% lidocaine without diluting to 4 mg/ml.
Kind regards,
Jeff
miguel says
when does the sodium bicarb injection needed to be administered and ladecian iv
Jeff with admin. says
Here is the AHA position on Sodium Bicarbonate:
Here is the AHA positions for Lidocaine:
Kind regards,
Jeff
Jeni says
We dose Epi as soon as possible. What is right? Should you wait to give epi after 2 cycles of cpr, or give it as soon as possible?
Jeff with admin. says
Technically, epinephrine should be given after the 2nd shock during CPR. (for pulseless VT/VF)
As long as the emphasis is on high-quality CPR and early defibrillation, it is ok to give the epinephrine asap. Just realize that AHA sets guidelines that are rigid for the purpose of standardization and in a real scenario if a dynamic team is working in coordination, things may be done simultaneously.
For the purposes of testing. Give epinephrine after the 2nd shock during CPR (pulseless VF/VT). According to the guidelines, epinephrine may be given asap for asystole and PEA.
owensnick11 says
The video says to give epi after the second shock and then every 3-5 minutes. But, then it says to give amniodarone after the 3rd shock. Are we giving epi and amniodarone at the same time if the epi is every 3 to 5 minutes or do we stop giving epi once we start giving the amniodarone?
Thanks
Jeff with admin. says
After the first dose of epinephrine, the epinephine is on its own time table and can be give every 3-5 minutes regardless of what antiarrhythmis are give after this. You can give the amiodarone and epinephrine back to back after the 3 shock. Or you could give the second dose of Epi after the 4th shock. There should be someone watching the time and calling out when the epi can be given. Make sure that you follow the epi with 20 ml of NS and also ensure that high quality CPR is being provided.
Kind regards,
Jeff