There are several other tachycardia rhythms that can be seen with both stable and unstable tachycardia. These rhythms include monomorphic ventricular tachycardia and polymorphic ventricular tachycardia both of which are wide-complex tachycardias.
Wide complex tachycardias are defined as a QRS of ≥ 0.12 second. Expert consultation should be considered with these rhythms.
These wide-complex tachycardias are the most common forms of tachycardia that will deteriorate to ventricular fibrillation.
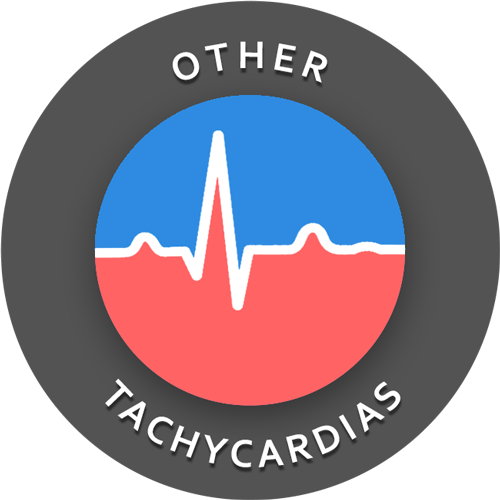
Monomorphic Ventricular Tachycardia
With monomorphic VT all of the QRS waves will be symmetrical. Each ventricular impulse is being generated from the same place in the ventricles thus all of the QRS waves look the same.
Treatment of monomorphic VT is dependent upon whether the patient is stable or unstable. Expert consultation is always advised, and if unstable, the ACLS tachycardia algorithm should be followed.
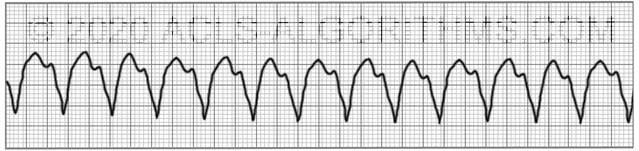
Polymorphic Ventricular Tachycardia
With polymorphic ventricular tachycardia, the QRS waves will not be symmetrical. This is because each ventricular impulse can be generated from a different location. On the rhythm strip, the QRS might be somewhat taller or wider.
One commonly seen type of polymorphic ventricular tachycardia is torsades de pointes. Torsades and other polymorphic VT are advanced rhythms which require additional expertise and expert consultation is advised.
If polymorphic VT is stable the ACLS tachycardia algorithm should be used to treat the patient. Unstable polymorphic ventricular tachycardia is treated with unsynchronized shocks (defibrillation). Defibrillation is used because synchronization is not possible.
These wide complex tachycardias tend to originate in the ventricles rather than like a normal rhythm which originates in the atria.
Top Questions Asked On This Page
-
Q: What are the doses for synchronized cardioversion?
A: Here are the cardioversion voltage doses:- Narrow regular: 50-100 J
- Narrow irregular: 120-200 J biphasic or 200 J monophasic
- Wide regular: 100 J
- Wide irregular: defibrillation dose (not synchronized)”
All of this information is covered on the tachycardia algorithm page.
-
Q: Is it necessary to memorize the doses listed above?
A: It is necessary to understand the concepts and be familiar with the shock dosages.
The repetition that is built into the website is designed to help you become very familiar with all of the concepts and use them in emergencies. -
Q: What sort of a pulse would you be feeling with a polymorphic VT?
A: You may feel a weak pulse or a strong pulse depending on how long the polymorphic VT has been going on. One thing is for sure….You won’t be feeling a pulse for very long if this rhythm continues.
Rolo says
if a patient has polymorphic VT a unsychronized shock is delivered but what is done after that? are we still on the tachycardia algorithm or the cardiac arrest (pvt/vf ) algorithm. Im not sure if this is right but i heard polymorphic VT is essentially VFIB and thought if you had that rhythm you are always on the cardiac arrest algorithm
ACLS says
Immediately after the shock, you would continue with CPR. After a round of CPR you would do a rhythm check and follow the appropriate algorithm depending on what the rhythm is.
Kind regards,
Jeff
Miriam Reyes Díaz says
Buen Día ,en la TV polimorfica estable se puede utilizar amiodarona o sulfato de magnesio ?
Saludos
Jeff with admin. says
It is very unlikely that polymorphic VT will be stable for a long period of time. In the case that it is, both magnesium and amiodarone would be appropriate antiarrhythmics to administer. Both can be given.
Kind regards,
Jeff
A Bradley BSN, MPH, NREMT-P says
You sure about that? Better make damn sure it’s not torsades. Amiodarone prolongs the QT interval, the kiss of death in torsades. If I’m unsure, I skip the amio and give lido instead. I would have somebody start a slow push of 2G mag while I charge the defibrillator…
ACLS says
With the presence of torsades, lidocaine would definitely be a better option. Thank you for pointing that out. Kind regards, Jeff
Andrew says
If a patient is in unstable Polymorphic V-Tach would you be able to cardiovert that? I just heard the changing morphology of the R-Waves would throw off the synchronization algorithm and it wouldn’t be able to sync. Has anyone else heard this?
Jeff with admin. says
It is likely that the defibrillator will not be able to synchronize with the patient’s rhythm for the reason you have stated. In this case, unsynchronized cardioversion (defibrillation) would be indicated.
Kind regards,
Jeff
Jude says
Do you give certificate at the end of the training?
Jeff with admin. says
At this time I do not offer a certificate at the end of training. I am in the process of obtaining CEU’s for training and will offer a certificate once this is in place.
Kind regards,
Jeff
Brenda Biancosino says
CEU’s will be fantastic! Thank you for all you do. This is my third time using your site. I must say it gets easier each time but I wouldn’t dream of recert without using your site.
Np.masilva@gamil.com says
Thanks all is very helpful. I have been a practicing NP for 22 yrs, last ACLS certification 2 yrs ago, going thru your rhythyms has helped tremendously.
Mil gracias
PS missed the monitor for this part other tachycardia rhythyms
Rocky58 says
Its confusing to me when im going to do synchronize cardioversion and unsynchronized cardioversion thanks
Jeff with admin. says
I have created a webpage that addresses the confusion that people have about this subject.
synchronized versus unsynchronized cardioversion
Kind regards,
Jeff
becheng53 says
Use cardioversion in unstable tachycardia patient
Use pacing in unstable bradycardia
Use shock in unstable VT , vfeb ,complete heart block?
Right or wrong?
Jeff with admin. says
Everything is correct except, you would pace complete heart block which is classified as bradycardia.
Kind regards, Jeff
Brenda Biancosino says
and for unstable Polymorph VT- Defib?
Jeff with admin. says
You would most likely have to perform defibrillation.
It is unlikely that the defibrillator will sync with the patient rhythm so this would make synchronized cardioversion an unlikely option.
Kind regards,
Jeff
EDNY says
Hi Jeff, can I ask for clarification from the two quotes in your above texts?
1) Treatment of monomorphic VT: “if unstable, the ACLS tachycardia algorithm should be followed.” Does that mean defib?
2) Treatment of polymorphic VT: “if polymorphic VT is stable the ACLS tachycardia algorithm should be used to treat the patient. ” Does this mean anti-arrhythmic meds such as amio?
Thanks!!
Jeff with admin. says
The answer to the first question is, No it does not mean defibrillation. In the case of unstable tachycardia, synchronized cardioversion should be used to convert the arrhythmia.
The answer to the second question is Yes, however, keep in mind that Torsades de Pointes may be caused by a magnesium deficiency and in this case, you would give magnesium first.
Cardioversion may be necessary if the arrhythmia persists.
Kind regards, Jeff
Sarath says
Thanks
Andy says
Wait, you can’t synch polymorphoc vtach or torsades…did you mean defib?
ACLS says
Thanks for pointing this out. I did mistakenly state cardioversion. Meant defib.
Thanks so much for the catch!
Kind regards,
Jeff
A Bradley BSN, MPH, NREMT-P says
Stay away from amio in PMVT!! You must be absolutely certain it’s not torsade. You will find out real fast if you have torsade after you give amiodarone; get the defib out because the pt’s pulse is going to go away, unresponsive, apneic etc.
jwoody1is says
Do you have any advice forall of who aren’t nurses but respiratory therapist. these HR rythms I have to go over everytime I take ALCS…. we don’t give the meds here so are also unfamiliar with dosages ect.?
Jeff with admin. says
If you use the interactive course guide to go through the material on the site, you will receive a thorough yet simplified review of all of the rhythms that you will encounter during ACLS, and it should be very sufficient to give you a full understanding of the rhythms and any medications used. Don’t get over concerned regarding medications. There are really only 4 medications you need to be familiar with for adult ACLS epinephrine, atropine, amiodarone, and adenosine. If you understand these 4, and you will if you complete the interactive course guide, you will be good to go. Kind regards, Jeff
Paramedic says
If a patient is in normal sinus rhythm with runs of VT and stable how do you treat them.
If a patient is in a normal sinus rhythm with runs of VT and unstable how would you treat them.
Jeff with admin. says
IV access, 12 lead ECG, Consider adenosine only if regular and monomorphic, Consider antiarrhythmic infusion. Most likely the antiarrhythmic infusion will be the best option. This patient needs to be in an ICU and under continuous monitoring.
In fact it would be wise to attached the patient to a defibrillator and keep it on at the bedside.
There are some variables here. Is the patient only unstable during the VT? What are the patient’s other symptoms?
Kind regards,
Jeff