Looking for PALS H’s and T’s go HERE.
Knowing the H’s and T’s of ACLS will help prepare you for any ACLS scenario. The H’s and T’s of ACLS is a mnemonic used to help recall the major contributing factors to pulseless arrest including PEA, Asystole, Ventricular Fibrillation, and Ventricular Tachycardia. These H’s and T’s will most commonly be associated with PEA, but they will help direct your search for underlying causes to any of arrhythmias associated with ACLS. Each is discussed more thoroughly below.
Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hyper-/hypokalemia, Hypoglycemia, Hypothermia.
Toxins, Tamponade(cardiac),Tension pneumothorax, Thrombosis (coronary and pulmonary), and Trauma.
The H’s include:
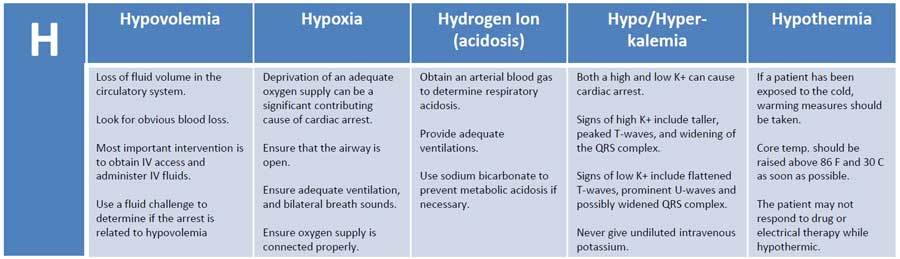
Hypovolemia
Hypovolemia or the loss of fluid volume in the circulatory system can be a major contributing cause of cardiac arrest. Looking for obvious blood loss in the patient with pulseless arrest is the first step in determining if the arrest is related to hypovolemia. After CPR, the most important intervention is obtaining intravenous access/IO access. A fluid challenge or fluid bolus may also help determine if the arrest is related to hypovolemia.
Hypoxia
Hypoxia or deprivation of adequate oxygen supply can be a significant contributing cause of cardiac arrest. You must ensure that the patient’s airway is open and that the patient has chest rise and fall and bilateral breath sounds with ventilation. Also, ensure that your oxygen source is connected properly.
Hydrogen ion (acidosis)
To determine if the patient is in respiratory acidosis, an arterial blood gas evaluation must be performed. Prevent respiratory acidosis by providing adequate ventilation. Prevent metabolic acidosis by giving the patient sodium bicarbonate.
Hyper-/hypokalemia
Both a high potassium level and a low potassium level can contribute to cardiac arrest. The major sign of hyperkalemia or high serum potassium is taller and peaked T-waves. Also, a widening of the QRS-wave may be seen. This can be treated in a number of ways which include sodium bicarbonate (IV), glucose+insulin, calcium chloride (IV), Kayexalate, dialysis, and possibly albuterol. All of these will help reduce serum potassium levels. Read more about hyperkalemia with cardiac arrest here.
The major signs of hypokalemia or low serum potassium are flattened T-waves, prominent U-waves, and possibly a widened QRS complex. Treatment of hypokalemia involves rapid but controlled infusion of potassium. Giving IV potassium has risks. Always follow the appropriate infusion standards. Never give undiluted intravenous potassium.
Hypoglycemia
Hypoglycemia or low serum blood glucose can have many negative effects on the body, and it can be associated with cardiac arrest. Treat hypoglycemia with IV dextrose to reverse a low blood glucose. Hypoglycemia was removed from the H’s but is still to be considered important during the assessment of any person in cardiac arrest.
Hypothermia
If a patient has been exposed to the cold, warming measures should be taken. The hypothermic patient may be unresponsive to drug therapy and electrical therapy (defibrillation or pacing). Core temperature should be raised above 86 F (30 C) as soon as possible.
The T’s include:
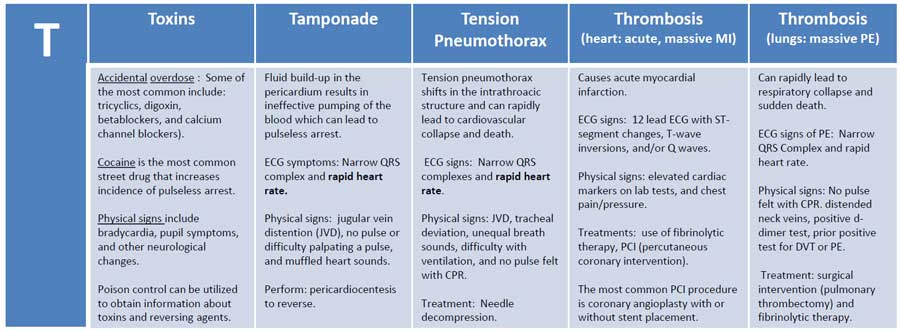
Toxins
Accidental overdose of a number of different kinds of medications can cause pulseless arrest. Some of the most common include tricyclics, digoxin, beta-blockers, and calcium channel blockers. Street drugs and other chemicals can precipitate pulseless arrest. Cocaine is the most common street drug that increases the incidence of pulseless arrest. ECG signs of toxicity include prolongation of the QT interval. Physical signs include bradycardia, pupil symptoms, and other neurological changes. Support of circulation while an antidote or reversing agent is obtained is of primary importance. Poison control can be utilized to obtain information about toxins and reversing agents.
Tamponade
Cardiac tamponade is an emergency condition in which fluid accumulates in the pericardium (sac in which the heart is enclosed). The buildup of fluid results in the ineffective pumping of the blood which can lead to cardiac arrest. ECG symptoms include narrow QRS complex and rapid heart rate. Physical signs include jugular vein distention (JVD), no pulse or difficulty palpating a pulse, and muffled heart sounds due to the fluid inside the pericardium. The recommended treatment for cardiac tamponade is pericardiocentesis.
Tension Pneumothorax
Tension pneumothorax occurs when air is allowed to enter the pleural space and is prevented from escaping naturally. This leads to a build-up of tension that causes shifts in the intrathoracic structure that can rapidly lead to cardiovascular collapse and death. ECG signs include narrow QRS complexes and rapid heart rate. Physical signs include JVD, tracheal deviation, unequal breath sounds, difficulty with ventilation, and no pulse felt with CPR. Treatment of tension pneumothorax is needle decompression.
Thrombosis (heart: acute, massive MI)
Coronary thrombosis is an occlusion or blockage of blood flow within a coronary artery caused by blood that has clotted within the vessel. The clotted blood causes an acute myocardial infarction which destroys heart muscle and can lead to sudden death depending on the location of the blockage.
ECG signs during PEA indicating coronary thrombosis include ST-segment changes, T-wave inversions, and/or Q waves. Physical signs include elevated cardiac markers on lab tests.
For patients with cardiac arrest and without known pulmonary embolism (PE), routine fibrinolytic treatment given during CPR has shown no benefit and is not recommended.
Treatments for coronary thrombosis before cardiac arrest include the use of fibrinolytic therapy, or PCI (percutaneous coronary intervention). The most common PCI procedure is coronary angioplasty with or without stent placement.
Thrombosis (lungs: massive pulmonary embolism)
Pulmonary thrombus or pulmonary embolism (PE) is a blockage of the main artery of the lung which can rapidly lead to respiratory collapse and sudden death. ECG signs of PE include narrow QRS Complex and rapid heart rate. Physical signs include no pulse felt with CPR. distended neck veins, positive d-dimer test, prior positive test for DVT or PE. Treatment includes surgical intervention (pulmonary thrombectomy) and fibrinolytic therapy.
Trauma
The final differential diagnosis of the H’s and T’s is trauma. Trauma can be a cause of pulseless arrest, and a proper evaluation of the patient’s physical condition and history should reveal any traumatic injuries. Treat each traumatic injury as needed to correct any reversible cause or contributing factor to the pulseless arrest. Trauma was removed from the T’s but is still to be considered important during the assessment of any person in cardiac arrest.
Stacey says
If you identify that the patient has a tension pneumothorax do you perform cpr prior to needle decompression or is it contraindicated?
ACLS says
You would want to do the needle decompression as soon as possible. CPR is not contraindicated but will unlikely be unsuccessful until needle decompression.
Kind regards,
Jeff
Elena Seitz says
Excellent ACLS Refresher: Perfect way to assess one’s strengths/weaknesses, and to brush up on any rusty knowledge/skills. Practical, authentic, and realistic. Organized and systematic format. Information accurate, and presented clearly and succinctly. Adeptly incorporates multiple teaching/learning approaches—e. g. Auditory; visual; video; visually-friendly graphics; printable material; downloadable material; tactile/hands-on action (multiple quizzes; practice code situation case scenarios); teach and teach-back techniques; emphasizes/reviews/repeats the most important info; includes specific page numbers from AHA ACLS book for those who seek additional details on topics/issues; includes Q & A with explanations and brief rationales.
Martín Roberto López López says
Gracias por compartir me a permitido mejorar mucho mi aprendizaje.
Thando says
Very informative
Samantha Lamplugh says
Why is Hypoglycemia taken off the list of H and Ts for reversible causes of arrest? Should IV dex be withheld until a ROSC is established? If so, why is that?
Thank you
ACLS says
I believe that hypoglycemia was removed for several reasons.
In several large studies, patients who received IV dextrose during the resuscitation attempt were significantly less likely to survive to hospital discharge when compared to patients who did not receive dextrose.
For those who did survive, administration of dextrose resulted in a greater risk of unfavorable neurologic outcome compared to the control group.
The same findings were also confirmed in animal studies.
Here are a couple of links to articles if you’re interested:
Article 1
Article 2
Article 3
Article 4
The administration of dextrose should be used with caution and is typically not recommended for the non-diabetic. No version of the guidelines recommends glucose administration unless hypoglycemia is suspected or confirmed.
I have not been able to find specific American heart Association documentation for the removal of trauma and hypoglycemia, but through a review of literature came to this conclusion. American heart Association does not make it easy to find or understand the reasoning for some of the changes that they make in the guidelines.
Hope this helps.
Kind regards,
Jeff
Khalid says
Good evening, now the patient in cardiac arrest, how to diagnose tension pneumothorax, P.E and if they are diagnosed what can be done during cpr?
Thanks
ACLS says
Identification: Tension pneumothorax is classically characterized by hypotension and hypoxia. On examination, breath sounds are absent on the affected lung and the trachea deviates away from the affected side. The thorax may also be hyperresonant; jugular venous distention and tachycardia may be present.
Treatment:
If the above symptoms are observed then the use of thoracostomy or needle decompression to treat the pneumothorax would be indicated.
Pulmonary embolism is more difficult to identify and treat. If it is suspected then fibrinolytic therapy would be indicated.
Kind regards, Jeff
Tatiana Guerra gonzalez says
ES UN SITIO IDEAL PARA PREPARARSE PARA EL ACLS GRACIAS JEFF
Lauren says
Why can’t you feel a pulse while performing CPR for patient’s with a PE or tension pneumothorax?
Jeff with admin. says
For PE the decreased ability to palpate a pulse is a result of the decreased volume of blood that reaches the heart with each contraction. The volume of blood reaching the heart is decreased and therefor the volume of blood that is ejected with compressions or cardiac contraction is reduced.
For tension pneumothorax the decreased ability to palpate a pulse is a result of the increased resistance created by the pressure of the tension pneumothorax against the pericardium. The heart’s blood volume capacity is decreased because of the tension pneumothorax. This ultimately decreases perfusion pressure which results in the decreased ability to palpate a pulse.
Kind regards,
Jeff
Faith says
Very usefull site
Dmitry says
Hello to everyone! What is rapid but controlled infusion of potassium in the presence of PEA caused by hypokalemia?
Jeff with admin. says
The scenario would not be very promising. Rapid infusion of potassium is not really that rapid and you’re going to need at least one hour to infuse up to 40 mEq. If potassium level is < 3 and the patient is symptomatic, 40 meq/hour may be administered to intensive care patients. Please let me know if you have any other questions. Kind regards, Jeff
Coy says
Oh my Gosh, max is 20 meqs/hour. More than that is called lethal injection.
Roberta Armstrong says
I find PEA the most confusing of all rhymes. Seems most tx is Labs {in hosp}
Jeff with admin. says
The most important aspect of treating PEA is to identify the cause of the PEA. If PEA is of a sudden onset, there should most likely be an identifiable and treatable cause.
The most important intervention is high-quality CPR. High-quality CPR will help give your time to determine the cause if it can be identified.
Kind regards,
Jeff
M says
A good note… Put a pulse oximeter on the patient. If you have a pulse you have a good chance of capturing a waveform.
Kenner says
In a recent case of a patient with PEA, in full arrest, epi was given x3 @ 7 minute intervals, 40 of vassopressin wasnt considered, while being transported via ambulance 4 minutes after arriving at the scene for OHCA. Thoughts?
ACLS says
The epinephrine should have been given at no more than five minute intervals. The half-life of epinephrine is approximately 2 minutes. The seven minute interval would be too long to maintain adequate threshold of epinephrine. Vasopressin is no longer used in ACLS guidelines.
Kind regards,
Jeff
DVK2485 says
Could not pass without this site Thanks for all your clarity and information
Jiringho Lilian says
Thanks for the information. I am a lecturer in school post basic Accident And Emergency Nursing ,Lagos University Teaching Hospital ,Lagos State ,Nigeria.
Lilian Jiringho.
DJackson says
Well stated, easy to look at while studying ACLS.
Ozhan Surer says
Thıs ıs the best online website program for ACLS preparation. I strongly recommend this program who prepare the ACLS exam, thoroughly covers all the topics. Thank you very much.