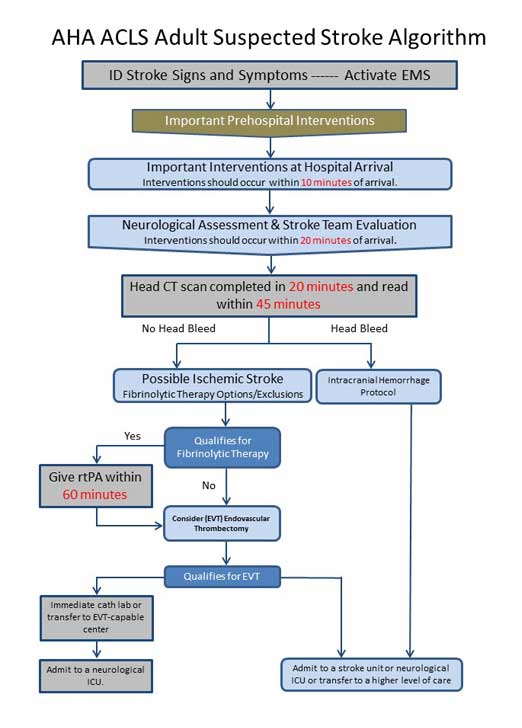
 The acute adult stroke diagram outlines all of the steps for assessment and treatment of ischemic stroke according to AHA guidelines. In the following pages the suspected stroke algorithm will be reviewed step-by-step.
The acute adult stroke diagram outlines all of the steps for assessment and treatment of ischemic stroke according to AHA guidelines. In the following pages the suspected stroke algorithm will be reviewed step-by-step.You can start here:
Before proceeding, you may also download and review the Suspected Adult Stroke Algorithm Diagram.
Download Stroke Diagram Here (This will open in a new window.)
Soumyamol Joy says
I have recently did my ACLS and successfully passed. At the start had no idea what is it all about and start practicing on for two weeks and passed the course. Simple and constructive way of teaching made everything easy and fun. Enjoyed the whole studies and will recommend to everyone. Thank you so much.
Jeff with admin. says
Hi Soumyamol,
Thanks for letting me know how things went. Great job. I’m so glad that the site was helpful for you. Kind regards, Jeff
SUSAN ISAAC says
Jeff,
Thank you, for clearing the doubt of giving aspirin.
So it’s given if the pt. is NOT a candidate for fibrinolytic therapy and there is NO hemorrhage.
regards,
Susan.
Jeff with admin. says
That is correct. If the patient is not a candidate for fibrinolytic therapy and there is no hemorrhage you would give them aspirin.
Kind regards,
Jeff
Stephanie Ahmadi says
What if ASA was already given outside of the hospital and they are otherwise a candidate for Fibrinolytic therapy?
ACLS says
The administration of aspirin in the prehospital setting would not change the status of the patient regarding being a candidate for fibrinolytic therapy. They could still be given fibrinolytic therapy.
Kind regards,
Jeff
Barbara Pezzengrilli says
I WORK IN A STROKE UNIT AND OF COURSE ASA WOULD NOT BE GIVEN IF THERE WERE A BLEED, BUT WHEN I LOOK AT THE ALGORITHM IT LOOKS AS IF IT IS PART OF THE HEMMORAGHIC TREATMENT. IT REALLY NEEDS TO BE CHANGED.
Jeff with admin. says
In the diagram, as indicated by the arrows, the ASA is only given to a patient that does not have a head bleed but do not qualify for fibrinolytic therapy. There is no arrow connecting ASA to the head bleed, and it would only be for non-head bleed patients that do not qualify for fibrinolytic therapy. Kind regards, Jeff
Lee Sherman says
Found above to be helpful, will use it to help r/o CVA and expedite tx when CVAs occur, thank you.
Rob Casserley says
Jeff
I am really unclear in the ACLS guidelines about thrombolysis in situations of ‘soft neurological defecit’, with otherwise all thrombolytic criteria fulfilled, eg – left arm and leg parasthesiae starting within 3 hours – with resolution of the arm symptoms after 2 hours but persisting leg altered sensation. Head CT no bleed. From the patient perspective there is a hard neuro defecit – harder to confirm objectively. Does this patient default to being a thrombolysable candidate(?) or as there is no m otor defecit, she is non-thrombolysable(?) or because she has shown signs of improvement already – should one postpone thrombolysis, even though there is a subjective hard neuro defecit? Risks vs benefits of thrombolysis etc…
Thanks for your feedback.
Additionally – do you feel that all CT heads should be with contrast these days. It is a hard argument to make with our radiologists – but would ssem to make sense when trying to ‘rule in’ thrombotic stroke
Best
Rob Casserley
Jeff with admin. says
I’m definitely not an expert or even experienced with stroke care protocol. I did run this by my brother how contributes to the site and is a critical care nurse specialist. He forwarded this stroke care protocol to me and thought that it might be helpful for you in your understanding.
Regarding the head CT. Currently in the United States, noncontrast computed tomography (CT) remains the primary imaging modality for the initial evaluation of patients with suspected stroke.
Kind regards,
Jeff
Sharon Draveling says
If a patient is already taking Aspirin 325mg/day or 81mg/day do you given an additional dose of Aspirin in the event of possible stroke or heart attack?
Jeff with admin. says
It is common practice to give an additional dose as part of the algorithm protocol. In this situation, the ASA may help and will not hurt. Kind regards, Jeff
shah707@hotmail.com says
In the stroke Algo,it suggests ASA in a patient with head bleed on the R side of the Algo-why?
Thx
Jeff with admin. says
The ASA is only given for the ischemic stroke patient who does not qualify for fibrinolytic therapy. These patients are treated in the same pathway as the hemorrhagic stroke patients but if you look closely, the ASA is not in the path that the hemorrhagic stroke patients take. It is on the side is is only reserved for the ischemic stroke patients who do not qualify for fibrinolytic therapy.
Kind regards,
Jeff
Mary DB says
A 80 year old female with a previous diagnosed haemorrhagic stroke 2 years back comes with recurrent TIA : should ASA be given as a part of treatment and also for prevention of recurrent strokes?
Jeff with admin. says
This patient would not be a candidate for fibrinolytic therapy, but ASA can be given as part of their treatment.
Kind regards,
Jeff
MARLON says
Hi Jeff, when do we need to add up antiplatelet like clopidogrel in ischaemic stroke? Will it not be necessary to give in early treatment? Thanks.
Jeff with admin. says
Clopidogrel is not a primary medication used within ACLS stroke protocol. Here is an article on the AHA Position for the use of clopidogrel in stroke patients.
iodine1859 says
Jeff, could you please tell me what the 8 D’s of stroke are; and the H’s and T’s of PEA?
Jeannie
Jeff with admin. says
Here is a page about the H’s and T’s of PEA: H’s and T’s of ACLS
Kind regards,
Jeff
http://www.acls-algorithms.com
Elaine12 says
I am not clear on the aspirin.So you give the ASA if the pt is not a candidate for fibrinolytic therapy,and there is no hemorrhage?
Jeff with admin. says
That is correct. You give ASA if the pt. is not a candidate for fibrinolytic therapy and there is no hemorrhage.
Kind regards,
Jeff
Jane says
Why is “give aspirin” listed under “head bleed” ?
Jeff with admin. says
If you look where the Aspirin on the algorithm, a head CT has already ruled out “head bleed” in he case that ASA is given. You are crossing over to the “right branch stroke hemorrhage pathway” at a later time in the algorithm and “head bleed” would have already been ruled out. Does that make sense?
Kind regards,
Jeff
nint says
Jeff..according to the stroke algorithm …would aspirin be administered for a hemorrhagic stroke? Doesn’t seem like this would be indicated.
Jeff with admin. says
Aspirin would not be administered for a patient with hemorrhagic stroke. This is discussed in Step 5 of the stroke algorithm, this is discussed. Here is the link: Step 5: Adult Stroke Algorithm
Kind regards,
Jeff