In this ACLS Megacode scenario, use the appropriate ACLS algorithms to treat the patient. There are 12 questions for this ACLS megacode scenario. Assume the use of biphasic defibrillator in all scenarios.
Quiz Summary
0 of 12 Questions completed
Questions:
Information
You have already completed the quiz before. Hence you can not start it again.
Quiz is loading...
You must sign in or sign up to start the quiz.
You must first complete the following:
Results
Results
0 of 12 Questions answered correctly
Time has elapsed
You have reached 0 of 0 point(s), (0)
Earned Point(s): 0 of 0, (0)
0 Essay(s) Pending (Possible Point(s): 0)
Categories
- Not categorized 0%
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
- 9
- 10
- 11
- 12
- Current
- Review
- Answered
- Correct
- Incorrect
-
Question 1 of 12
1. Question
A 40-year-old man arrives at the ER accompanied by his family. He is complaining of palpitations after working outside for several hours. The assessment is as follows:
SKIN: Hydrated, pale, warm and dry
CVS: Strong peripheral pulses and a BP of 125/80
CNS: Fully intact
RESP: RR is 22, no resp. difficulties, lungs CTAYou start an IV on the patient. The monitor shows a narrow complex SVT (160).

What is your next intervention?
CorrectIncorrect -
Question 2 of 12
2. Question
You have performed vagal maneuvers. This is what you see on the monitor:
What is your next step?CorrectIncorrect -
Question 3 of 12
3. Question
You give 6mg Adenosine rapid IV push with no effect. 12mg Adenosine rapid IV push is then given. The patient develops severe chest pain, his rhythm is the same, and his vital signs are: HR 220, BP (not obtainable), and weak pulse. The patient also has LOC changes. Your next step should be?
CorrectIncorrect -
Question 4 of 12
4. Question
After synchronized cardioversion is unsuccessful, the pt. continues to deteriorate. The patient is now unconscious with pulseless ventricular tachycardia. Below is what you see on the monitor:
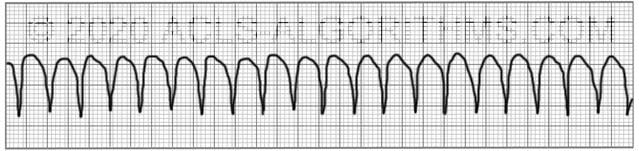
What is the first and most important intervention?
CorrectIncorrect -
Question 5 of 12
5. Question
You perform defibrillation with 120 J. What is your next intervention?
CorrectIncorrect -
Question 6 of 12
6. Question
After completing 5 cycles of CPR, the rhythm is unchanged. You shock a second time with 200 J and resume CPR. While completing the cycle of CPR what else should be done?
CorrectIncorrect -
Question 7 of 12
7. Question
You have given the epinephrine and completed the 5 cycles of CPR. A rhythm check reveals no change. You attempt a third defibrillation. What will be your defibrillator setting?
(In all scenarios, assume that the biphasic defibrillator shock setting can be from 50-360 Joules. The shock selection on many biphasic defibrillators can vary.)CorrectIncorrect -
Question 8 of 12
8. Question
The third shock is delivered and you restart CPR (5 cycles). What medication should be given after the 3rd shock during CPR?
CorrectIncorrect -
Question 9 of 12
9. Question
What is the correct dosing for amiodarone in the Cardiac Arrest Algorithm?
CorrectIncorrect -
Question 10 of 12
10. Question
You give amiodarone 300 mg (first dose) and finish the cycle of CPR. Upon a rhythm check, you see, the patient has converted to a normal sinus rhythm and has a pulse (ROSC). As you begin the post-arrest phase, the patient has a short run of VT. In light of the continued arrhythmia, you are instructed to start an amiodarone drip for post-resuscitation maintenance therapy. What is maximum cumulative dose for amiodarone in a 24 hour period?
CorrectIncorrect -
Question 11 of 12
11. Question
Lidocaine can be used instead of amiodarone as an antiarrhythmic during cardiac arrest. What is the proper dosing of lidocaine?
CorrectIncorrect -
Question 12 of 12
12. Question
Great Job! You saved the patient He has been stabilized and intubated, but does not respond to verbal commands. He is transported to the hospital's ICU. Since the patient is not responsive what would be the most important intervention in the post-cardiac arrest phase.
CorrectIncorrect
Jennifer L Williams says
It said HR 220 unobtainable BP. I took it as still has a pulse but deteriorating.
Emily L says
If the patient has an unstable tachyarrhythmia then the first intervention is immediate synchronized cardioversion
Rotchiel Flotlin says
Patient is unresponsive and PULSELESS. … Isnt we give CPR ?
ACLS says
Because this was a witness cardiac arrest and the patient is connected to the defibrillator, the first intervention should be defibrillation. Kind regards, Jeff
SETH JECHIE KELLY says
YES you have to begin CPR every unresponsive patient without pulse or you are unable to detect pulse with 10 seconds initiate chest compression
BFD081 says
Where exactly in ACLS do we perform 5 rounds of CPR without 2 minute rhythm checks?
ACLS says
Within the framework of ACLS during cardiac arrest, after five cycles of CPR (two minutes) always perform a rhythm check.
Kind regards,
Jeff
Santhi a/p Chinniah says
Very good and increase my knowledge in my nursing carrier
jai qlate says
please explain to me regarding the post cardiac arrest ROSC, why we need to maintain the pt temperature?
my second question, what the normal range for temperature pt in intubated condition.
Jeff with admin. says
You can find a review of the post cardiac arrest information here: Post cardiac arrest care review
The normal ranges are discussed in section as well.
If you need more information, you can find it here: AHA post cardiac arrest
Kind regards,
Jeff
Hazem Azzam says
Induced hypothermia just for 24 hrs for patients post cardiac arrest will decrease the metabolism rate then will help in decreasing the consumption of oxygen then will decrease the workload of the heart. It is like preserving energy of the heart after arrest.
Lissa Barnes says
It is also neurologically supportive
Bill says
jai qlate, I am a resident physican at UCLA John Hopkins. I am on my upteennth round of ACLS/PEDACLS renewals in my long and storied career as a Emergency/Cardiology Physician Specialist…
Now, regarding your two part question:
1. The temperature needs to be maintained at this point post resuscitation for a couple reasons.. Remember, we have now restored normal sinus rhytmn, but during this one of many unique emergency trauma scenarios, a couple things happened. The obvious point is that heat loss occurred and the core temperature likely dropped, In in case, we would like to prevent any further cyanosis (ABG chemistry imbalance) and subsequent tissue damage (brain, heart, especially). If you could imagine the situation in real life, not only do we have a patient who has unregulated breathing, but also even during the resuscitation process, heat loss very may well occur as well, as the elements (mind you, I work in emergency now, so I do not know your background, so apologies for that) can be unpredictable in these situations.
2. regarding the actual temp during intubation, of course the same homeostatic principles apply. … I’m not sure how to best answer that question.. but you can certainly reach out if you need any further assistance.
Billy.Chan@aol.net
Good luck on your journey of the art and science of EM medicine.
SETH JECHIE KELLY says
In ROSC Targeted temperature management simply called TTM it the safe and effective strategy to grant that patient in a comatose a neuroprotection and to to alleviate mortality and improve neurological outcomes in unresponsive patients who achieve ROSC after cardiac arrest.
in the second question, there is no specific temperature range for patient in intubated condition but rather patient who gain ROSC and under TTM is perform under 32-36 degrees Celsius
Seth Jechie Kelly
Mayflor Altamira says
Good day..pls show me the difference between monomorphic ventricular tachycardia and polymorphic ventricular tachycardia.i thought question no.3 would be answered perform early defibrillation defibrillation.now I’m confused.pls help..
Jeff with admin. says
In question 3, what is important is not the difference between monomorphic and polymorphic in this situation. The important difference is that the patient is unstable. Any unstable tachycardia whether monomorphic or polymorphic requires immediate synchronize cardioversion.
In question number 4, once the patient is pulseless then what is important is immediate defibrillation. It doesn’t matter whether the ventricular tachycardia is monomorphic or polymorphic.
Kind regards,
Jeff
Gina Thompson says
Hello Jeff,
Can unstable polymorphic tachycardia be successfully treated with synchronized cardioversion, how do we sync on the R with so many variations in this rhythm?
Jeff with admin. says
It is unlikely that the defibrillator will synchronize with polymorphic ventricular tachycardia. When you attempt synchronization, the machine will promptly tell you that synchronization is not possible.
In that situation, you should revert to manual unsynchronized defibrillation.
Kind regards,
Jeff
Tom says
For number 3, the key is that the shock be synchronized because there still are pulses.
David Quatrochi says
Hi Jeff,
I know different agencies have different protocols. Our protocols changed about 2 years ago for Adenosine. Used to be 6mg 12mg 12mg for Adenosine. Our protocol is 12mg , may repeat 1 time (Denver Metro Protocol).
Thanks, Dave Q
Jeff with admin. says
That sounds like a fine protocol. I have seen 6 mg fail many times and 12 mg usually does the trick. Remember, the American Heart Association guidelines are just guidelines. A lot of different emergency units develop protocols that deviate in small ways from American heart guidelines and this is fine.
AHA still says give 6mg if it fails then give 12 mg.
Kind regards,
Jeff
crslmrn says
Great site, Jeff!
this is my 3rd or 4th review on this site, I was always successful with my recertification. My next recertification is 9/9/18 and I am confident that I will be successful after my review.
Thank you!!
Christine
johnathan montgomery says
Question number 3. Should be an immediate defibrillation with unstable vtach. Synch Cardioversion is for your unstable atrials
Jeff with admin. says
Your statement is incorrect. Per the tachycardia algorithm, any monomorphic regular unstable tachycardia should receive synchronized cardioversion.
Defibrillation is reserved for pulseless ventricular tachycardia, ventricular fibrillation and polymorphic ventricular tachycardia. Unstable Polymorphic ventricular tachycardia will receive unsynchronized cardioversion due to the fact that synchronization cannot occur with polymorphic ventricular tachycardia.
Kind regards,
Jeff
Ahmed Al Jahwary says
Excellent scenarios: but there should be sequential and complete each on its own before they are made to change to worse. If pt has palpitation and found to have SVT IN SINUS RHYTHM then let us complete that to the end with its all necessary details WHY change it to VF or VT (these should be allocated on their own different scenarios with all their associated procedures). There could be some cases that are purposely made to deteriorate BUT after finishing all individual scenarios.
Elayne says
Thanks, I have the same opinion. That was the part I struggled and get confuse. Today is the skill/ training part and I nervous . …hope this not interfere.
Jeff with admin. says
Hi Elayne,
I do plan on developing a series of simplified megacode simulations that go through each sequence with the algorithms. I do appreciate the feedback. Kind regards, Jeff
César Eduardo Pérez Millán says
Excelente práctica!! Muy educativa
Manidra Ghosh says
Great run of challegs.
atul says
excellent site